

CBC and CBD are both non-psychoactive cannabinoids made by the cannabis plant from the same precursor (CBGA). They’re often marketed as interchangeable “minor cannabinoids for inflammation.” They’re not interchangeable. CBC hits the TRPA1 pain/inflammation receptor harder than any other cannabinoid. CBD is a negative allosteric modulator at CB1 with broad effects at serotonin, TRPV1, and FAAH pathways. CBD has FDA-approved Epidiolex and decades of human research. CBC has zero human clinical trials as of April 2026. They do have one direct head-to-head study (Grogan et al. 2023 in Annals of Plastic Surgery), which tested them alone and in combination in a mouse arthritis model. The combination outperformed either one alone. This guide runs the full side-by-side: chemistry, receptor pharmacology, clinical evidence, use cases, dosing, cost, and when to choose each.
🧪 Lab Tested | 👩💼 Woman-Owned | 🏆 Est. 2017
Table of Contents
- The Short Answer
- What Is CBC?
- What Is CBD?
- Chemistry and the Shared Biosynthetic Parent
- Receptor Pharmacology Side-by-Side
- Clinical Evidence: CBD’s Depth vs CBC’s Preclinical-Only Status
- The Grogan 2023 Direct Head-to-Head
- Pain: TRPA1 vs TRPV1 Mechanisms
- Inflammation: Both Have Preclinical Data
- Anxiety: CBD Only
- Epilepsy: CBD Only (FDA-Approved)
- Skin and Acne: CBC’s Unique Edge
- Combining CBC and CBD
- Dosing Research vs Commercial Reality
- Side Effects and Drug Interactions
- Cost, Availability, Legal, and Drug Tests
- Decision Framework: Which Should You Use?
- Frequently Asked Questions
- Shop TribeTokes
CBC vs CBD at a Glance
| Psychoactive? | Neither. Both non-intoxicating at typical doses |
| Shared origin | Both derive from CBGA via plant biosynthesis (CBGA → CBCA → CBC; CBGA → CBDA → CBD) |
| CB1 interaction | CBC: weak partial agonist. CBD: negative allosteric modulator (Laprairie 2015) |
| Distinctive receptor | CBC: TRPA1 (most selective cannabinoid; EC50 ~90 nM). CBD: 5-HT1A + FAAH inhibition |
| Human clinical trials | CBC: zero. CBD: dozens plus FDA-approved Epidiolex |
| FDA-approved drug | CBC: none. CBD: Epidiolex (2018, for epilepsy) |
| Direct head-to-head data | Grogan et al. 2023, Annals of Plastic Surgery: CBC+CBD combination outperformed either alone in mouse arthritis |
| Pain mechanism | CBC: TRPA1 + CB1 + adenosine A1 (Maione 2011). CBD: TRPV1 desensitization + anandamide |
| Plant abundance | CBC: typically <1% in flower. CBD: dominant in hemp |
| Cost per mg | Similar, both premium minor cannabinoids. CBC slightly higher on average |
The Short Answer
If you need the one-paragraph version: CBD is the well-studied, FDA-validated, evidence-rich cannabinoid with broad human data. CBC is the preclinical-only cannabinoid with genuinely interesting receptor pharmacology (particularly at TRPA1) but no human clinical trials. They share a biosynthetic origin (both come from CBGA), they’re both non-psychoactive, and they can be combined. One 2023 study directly tested both alone and together in a murine arthritis model, finding that the combination outperformed either compound alone. That’s the closest thing to a head-to-head comparison we have.
Practically: if you want a well-characterized cannabinoid for anxiety, sleep, or general wellness, choose CBD. If you’re specifically interested in CBC’s TRPA1-driven anti-inflammatory and analgesic research signals and willing to accept that consumer effects aren’t human-validated, choose CBC. If you want to try the Grogan 2023 combination approach for inflammation, CBC+CBD products are an option. The rest of this guide goes through each use case with sources.
What Is CBC?
Cannabichromene (CBC) is a minor cannabinoid produced by the cannabis plant in small amounts, typically less than 1% of total cannabinoids in mature flower. It’s derived from CBGA (the “mother cannabinoid”) through enzymatic conversion during plant maturation. CBC is non-psychoactive, binding the CB1 cannabinoid receptor only weakly.
What makes CBC pharmacologically distinctive is its activity at the TRPA1 channel (ankyrin-type transient receptor potential channel type 1). CBC is the most potent and selective TRPA1 agonist among non-psychoactive cannabinoids, with an EC50 around 90 nanomolar. TRPA1 is a validated target for human pain research, and CBC’s activity there is the pharmacological basis for its analgesic and anti-inflammatory research signals. For the full CBC picture including the preclinical evidence across anti-inflammatory, analgesic, antidepressant, neurogenic, and antibacterial effects, read our CBC benefits guide.
What Is CBD?
Cannabidiol (CBD) is the most studied non-psychoactive cannabinoid in cannabis. It’s the dominant cannabinoid in hemp by design: federal hemp status requires less than 0.3% delta-9 THC by dry weight, and CBD-dominant cultivars are the commercial norm. CBD research has an enormous head start on CBC, with thousands of papers, multiple systematic reviews, and one FDA-approved prescription drug.
CBD’s pharmacology is multi-target. A 2015 study by Laprairie and colleagues in the British Journal of Pharmacology (PMID 26218440) showed CBD acts as a negative allosteric modulator at CB1, binding a different site than THC does and reducing receptor activation by other ligands. CBD also agonizes 5-HT1A serotonin receptors, interacts with TRPV1 and GPR55, and inhibits the FAAH enzyme that breaks down anandamide. CBD has FDA approval as Epidiolex (2018) for seizures associated with Dravet syndrome, Lennox-Gastaut syndrome, and tuberous sclerosis complex. For the full CBD picture including the compound-level comparison with THC, see our CBD vs THC guide.
Chemistry and the Shared Biosynthetic Parent
CBC and CBD share a biosynthetic parent. The cannabis plant first synthesizes CBGA (cannabigerolic acid), the acidic precursor to all major cannabinoids. As the plant matures, specialized enzymes convert CBGA into three different acidic cannabinoids: THCA, CBDA, and CBCA. THCA becomes THC with heat. CBDA becomes CBD. CBCA becomes CBC.
So CBC and CBD are biosynthetic siblings, both produced from the same CBGA precursor via different enzyme pathways. Their molecular structures differ in how the central ring system is arranged, which explains their different receptor binding profiles. Both are polyphenolic cannabinoid scaffolds with alkyl side chains and no nitrogen. Both are lipophilic (fat-soluble), which affects bioavailability across delivery methods (covered in our CBD bioavailability guide; the same principles apply to CBC).
One key structural difference: CBC has a chromene ring closure that CBD doesn’t have, and CBD has an open ring feature that CBC lacks. These small structural differences explain why CBC is a potent TRPA1 agonist while CBD is not, and why CBD acts as a negative allosteric modulator at CB1 while CBC behaves differently at the same receptor.
Receptor Pharmacology Side-by-Side
This is where CBC and CBD differ most clearly. They overlap on some targets but have distinct primary mechanisms.
| Receptor / Enzyme | CBC Activity | CBD Activity |
| TRPA1 channel | Potent selective agonist (EC50 ~90 nM) | Minimal activity |
| CB1 cannabinoid receptor | Weak partial agonist | Negative allosteric modulator (Laprairie 2015) |
| CB2 cannabinoid receptor | Partial agonist activity | Indirect activity |
| TRPV1 | Moderate activity | Agonist / desensitizer |
| 5-HT1A serotonin | Not primary target | Agonist (well characterized) |
| Adenosine A1 receptor | Involved in CBC analgesic effect (Maione 2011) | Minimal direct activity |
| FAAH inhibition | Weak | Notable (raises anandamide levels) |
| MAPK pathway | Activated in anti-inflammatory action | Activated in some contexts |
The key takeaway: TRPA1 is CBC’s signature pharmacology. The 2024 therapeutic review by Sepulveda and colleagues in the Journal of Pharmacology and Experimental Therapeutics (volume 391, issue 2, pages 206-213) highlights this as CBC’s most distinctive activity. TRPA1 agonism drives CBC’s analgesic, anti-inflammatory, and gut-motility effects in preclinical models. CBD’s signature pharmacology is the CB1 negative allosteric modulation combined with 5-HT1A agonism and FAAH inhibition. Two different receptor toolkits, two different functional profiles.
Clinical Evidence: CBD’s Depth vs CBC’s Preclinical-Only Status
The clinical evidence gap is the most important contextual fact in this comparison.
CBD’s evidence base
- FDA-approved drug: Epidiolex (plant-derived CBD) approved in 2018 for Dravet syndrome, Lennox-Gastaut syndrome, and tuberous sclerosis complex seizures. Approval required multiple randomized placebo-controlled trials
- Anxiety and sleep: Shannon et al. 2019 in The Permanente Journal (PMID 30624194, N=72, case series), plus additional smaller randomized trials
- Pharmacokinetics: Millar et al. 2018 systematic review in Frontiers in Pharmacology analyzed 24 human pharmacokinetic studies
- Safety: WHO Expert Committee on Drug Dependence 2018 concluded pure CBD has good safety and no abuse potential
- Thousands of additional animal and human studies across multiple therapeutic areas
CBC’s evidence base
- Zero human clinical trials published as of April 2026
- 2024 authoritative review: Sepulveda et al. in the Journal of Pharmacology and Experimental Therapeutics concluded CBC shows “promising therapeutic potential” but emphasized “further studies are needed to conclusively determine its safety and efficacy in humans”
- Preclinical anti-inflammatory: Multiple in vivo and in vitro studies including Romano 2013 (murine colitis), carrageenan edema models
- Preclinical pain: Maione 2011 (Br J Pharmacol) demonstrated CBC analgesia in rats via TRPA1/CB1/adenosine A1
- Preclinical antidepressant: El-Alfy 2010 forced swim test (single study)
- Preclinical neural stem cells: Shinjyo & Di Marzo 2013 (PMID 23941747)
- In vitro skin: Oláh 2016 human sebocyte study
This lopsided evidence base is the most important thing to understand when comparing CBC and CBD. CBD has been studied thoroughly enough that it received FDA approval for a specific indication. CBC has interesting preclinical data but no human safety or efficacy trials. That doesn’t make CBC research worthless. It means decisions about CBC carry an evidence-quality caveat that decisions about CBD don’t carry to the same degree.
The Grogan 2023 Direct Head-to-Head
Here’s the one exception to the “no head-to-head data” gap. In 2023, Grogan and colleagues published “The Mechanism of Cannabichromene and Cannabidiol Alone Versus in Combination in the Alleviation of Arthritis-Related Inflammation” in Annals of Plastic Surgery (volume 90, 6S supplement 4, pages S408-S415, PMID 37332213, DOI 10.1097/SAP.0000000000003547). This is the only published direct CBC vs CBD comparison study.
Study design
- Murine collagen-induced arthritis model
- 48 mice initially enrolled, 35 completed the full study
- Three active treatment arms: CBC alone, CBD alone, and CBC+CBD combination
- Outcomes measured over 3 to 5 weeks: paw swelling, body weight, cytokine/chemokine gene expression
Key findings
- CBC alone: Mice treated with CBC showed significant weight gain between weeks 3 and 5, without a standalone anti-swelling advantage over control
- CBD alone: Modest cytokine correlations with arthritis markers, but no significant reduction in swelling compared to control
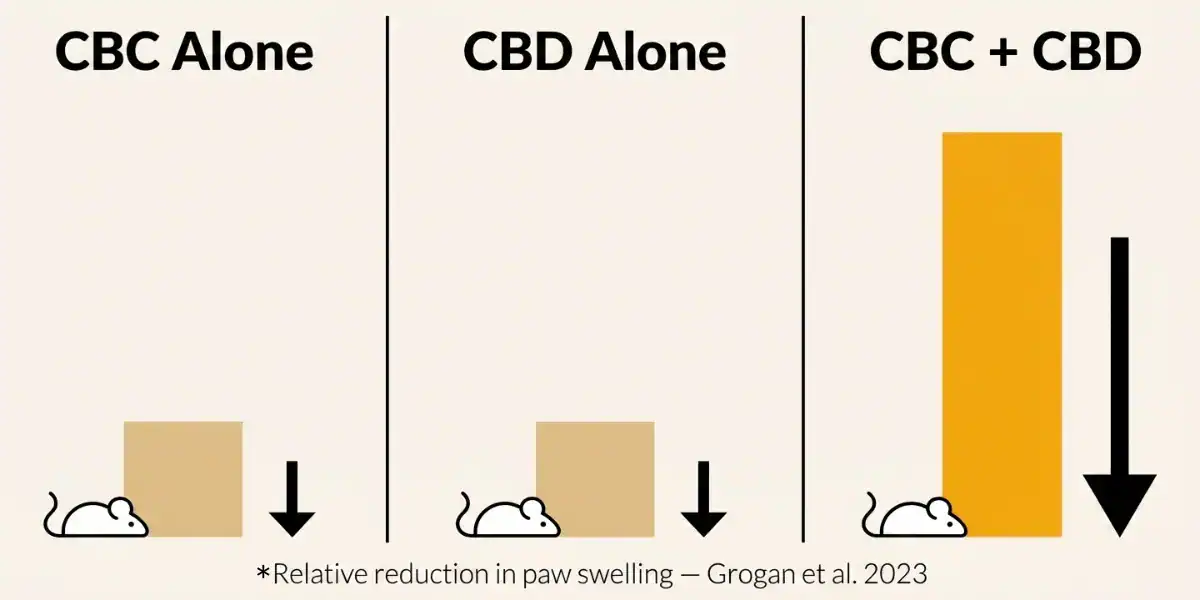
- CBC+CBD combination: Mice showed a significant decrease in swelling between weeks 3 and 5 compared to control, outperforming either compound alone
- Mechanism signals: The combined treatment affected eotaxin and lipopolysaccharide-induced CXC chemokine expression patterns
What this means practically
This is a small animal study, not a randomized human trial. But it’s the only published study that tested CBC alone, CBD alone, and the combination side by side. The result that the combination outperformed either alone has face validity given the different receptor systems each compound engages (CBC at TRPA1; CBD at CB1, 5-HT1A, TRPV1). If you’re considering CBC and CBD for inflammation-related use cases, Grogan 2023 is the best available evidence for trying the combination rather than picking one.
Honest caveat: the study used murine arthritis, not human inflammatory conditions. Translation to humans isn’t automatic, and no human RCT has confirmed the combination finding.
Pain: TRPA1 vs TRPV1 Mechanisms
Both cannabinoids have preclinical pain data, but through different pathways.
CBC for pain
Maione et al. 2011 in the British Journal of Pharmacology tested CBC analgesic effects in anesthetized rats. The study used intra-periaqueductal grey injection and measured tail-flick latency along with ventrolateral periaqueductal grey neuron recordings. CBC produced analgesic effects at 6 nmol, and the effect was antagonized by selective antagonists of CB1, adenosine A1, and TRPA1 receptors (but not TRPV1). This established CBC as a TRPA1-dominant analgesic with CB1 and adenosine A1 involvement.
CBD for pain
CBD’s analgesic mechanism operates through TRPV1 desensitization (chronic TRPV1 stimulation leads to loss of pain sensitivity), anandamide elevation via FAAH inhibition, and indirect CB1 effects through allosteric modulation. CBD has more human pain data than CBC, including observational studies and some RCT evidence for neuropathic and musculoskeletal pain, though the effect sizes are modest and results are mixed across studies.
Practical implication
CBC’s TRPA1 mechanism is the more novel pharmacology and might produce different effects than CBD in pain that’s driven by TRPA1-sensitive pathways (inflammatory pain, some neuropathic pain). CBD has more broadly documented pain utility across more pain types. If your goal is a specific inflammatory pain complaint, CBC may have mechanistic appeal; the Grogan 2023 arthritis finding fits this pattern. If your goal is general pain support with the best-characterized safety profile, CBD is the established choice.
Inflammation: Both Have Preclinical Data
Anti-inflammatory activity is the most-studied therapeutic area for both cannabinoids, though with different mechanistic signatures.
CBC anti-inflammatory
Romano et al. 2013 in the British Journal of Pharmacology demonstrated CBC reduced nitric oxide production in LPS-stimulated macrophages and ameliorated murine colitis in a DNBS model. Additional in vivo work has shown CBC reduces carrageenan-induced paw edema with reduction in iNOS, IL-1β, IL-6, and TNF-α at both mRNA and protein levels. The mechanism appears to involve MAPK pathway activation with CB1, CB2, and TRPA1 involvement depending on the preparation.
CBD anti-inflammatory
CBD has a parallel but larger body of evidence covering colitis, neuroinflammation, arthritis, and inflammatory skin conditions. Mechanisms span CB2 receptor engagement (indirectly), FAAH inhibition, PPAR-gamma activity, and 5-HT1A signaling. Human data is limited for direct inflammation endpoints but exists for conditions with inflammatory components.
Combination effect (Grogan 2023)
As discussed above, the Grogan 2023 arthritis model is the one direct test of CBC alone vs CBD alone vs combination. The combination outperformed either alone for swelling reduction. This suggests complementary anti-inflammatory mechanisms that pair usefully, at least in the mouse model.
Anxiety: CBD Only
CBD has human data for anxiety. CBC does not.
CBD’s anxiety evidence includes Shannon 2019 (N=72 open-label, 79.2% improved month 1), smaller placebo-controlled trials showing acute anxiety reduction at doses from 25-600mg, and decades of reports of subjective anxiety-reducing effects. The mechanism plausibly involves 5-HT1A agonism combined with allosteric CB1 modulation.
CBC has no human anxiety data and no animal model data specifically measuring anxiety-related behaviors as a primary outcome. El-Alfy 2010 tested CBC in the forced swim test (a depression model) but not in validated anxiety models like elevated plus maze or light-dark box. If anxiety is your goal, CBD is the cannabinoid with supporting evidence, and CBC is not currently a data-supported choice for this use.
Epilepsy: CBD Only (FDA-Approved)
Epilepsy is CBD’s strongest documented therapeutic use by a wide margin. Epidiolex (plant-derived CBD) was FDA-approved in 2018 for seizures associated with Dravet syndrome and Lennox-Gastaut syndrome, later expanded to tuberous sclerosis complex. Approval required multiple randomized controlled trials with placebo comparison at prescription doses (typically 5-20 mg/kg/day).
CBC has some preclinical anticonvulsant signals. A 2021 study cited in the Sepulveda 2024 review (Anderson et al., in the Scn1a-deficient mouse model of Dravet syndrome) found CBC was as effective as CBD at reducing seizures in that specific model. CBC was also effective in zebrafish seizure models at lower doses than CBD required. However, CBC was ineffective in electroshock-induced seizure tests, suggesting its anticonvulsant activity may be specific to certain seizure types rather than broadly effective.
None of that rises to the level of human validation. For seizure disorders, CBD via Epidiolex under medical care is the evidence-supported path. CBC is not an alternative here.
Skin and Acne: CBC’s Unique Edge
One area where CBC has notably more targeted research than CBD is acne and skin. Oláh et al. 2016 (PMID 27094344) tested several non-psychotropic cannabinoids including CBC, CBDV, CBG, CBGV, and THCV on human sebocytes (sebum-producing skin cells).
Key findings: CBC suppressed basal sebaceous lipid synthesis, reduced arachidonic acid-induced acne-like lipogenesis, and produced anti-inflammatory effects in sebocytes. The authors explicitly concluded that CBC “shows promise” as an anti-acne agent, placing it among a small group of cannabinoids with this specific research signal.
CBD has broader skin research and some acne-relevant evidence, but CBC’s sebocyte-specific data is a distinctive piece of the puzzle. For skin-targeted topical products, CBC may have a mechanism-backed case that CBD doesn’t share in exactly the same form. Topical products, of course, have different pharmacokinetic considerations than oral or inhaled cannabinoids.
Combining CBC and CBD
The Grogan 2023 study directly supports combining CBC and CBD for inflammatory applications, at least in the mouse arthritis model. The combination outperformed either compound alone.
Mechanistically, the case for combination is reasonable: CBC engages TRPA1 and CB2 (plus some CB1) while CBD acts at CB1 (as NAM), 5-HT1A, TRPV1, and FAAH. Different receptor systems could produce complementary rather than redundant effects. That’s a different pattern than CBD+CBN for sleep, where the 2024 Bonn-Miller RCT found that adding CBD to CBN did not augment sleep effects.
Honest caveats: the Grogan study is murine, not human. The mechanism of the combination synergy isn’t fully worked out. And outside of inflammation specifically, no other direct combination study has been published. If you want to experiment with CBC+CBD, inflammation-related goals have the best supporting evidence. For other goals, it’s reasonable to try but not evidence-backed.
Dosing Research vs Commercial Reality
| Use Case | CBC Research Reference | CBD Research Reference |
|---|---|---|
| Anxiety (human) | No data | 25-600mg depending on study (Shannon 2019 used 25-175mg/day) |
| Epilepsy (prescription) | Not applicable | 5-20 mg/kg/day (Epidiolex) |
| Inflammation (animal) | ~10-20 mg/kg mouse (various) | Varies by model and endpoint |
| Combination arthritis (animal) | Grogan 2023 tested both alone and together in mouse collagen arthritis model | |
| Human equivalent doses | Not established | Partially established for CBD (varies by use case) |
| Typical commercial dose | 2-10mg per serving | 10-50mg per serving |
Commercial reality: both cannabinoids tend to be under-dosed relative to research-effective doses in many consumer products. This is more pronounced for CBC given how new it is to consumer markets. If you’re trying to replicate the Grogan 2023 combination effect, you’d want products dosed meaningfully in both CBC and CBD per serving, which is uncommon at typical commercial dosages.
For bioavailability differences by delivery method that apply to both cannabinoids, see our CBD bioavailability guide.
Side Effects and Drug Interactions
Both cannabinoids have relatively mild side effect profiles, with different levels of characterization.
CBD
- Drowsiness, fatigue, decreased appetite at higher doses
- Diarrhea in a subset of users, especially at 200+ mg/day
- Drug interactions: CBD inhibits CYP3A4 and CYP2C9, which metabolize many prescription medications. Well-characterized concern
- WHO 2018 confirmed good safety profile and no abuse potential in pure form
CBC
- Less-characterized safety profile because of the zero-human-trial status
- Animal studies at research doses have not flagged significant adverse events
- Possible mild dry mouth, possible drowsiness at higher doses (anecdotal)
- Drug interactions: CBC interacts with ABCG2 and ABCB1 drug transporter proteins (tested in vitro), which could theoretically affect distribution of co-administered medications. CYP450 interaction potential is plausible but less studied than CBD’s
- Recommendation: if you take prescription medications, ask your doctor before starting CBC
Cost, Availability, Legal, and Drug Tests
Cost-wise, CBD is the cheapest, most widely available cannabinoid in the consumer market. CBC costs more per milligram because it’s present in much smaller amounts in the plant and requires either CBC-dominant strains or chromatographic isolation. The gap is meaningful: a given CBC dose typically costs 3 to 8 times more than an equivalent CBD dose.
Legally, both cannabinoids are federally legal in the United States under the 2018 Farm Bill, provided source plants stay under 0.3% delta-9 THC by dry weight. Both are sold openly in most states. The November 12, 2026 federal hemp redefinition (H.R. 5371 Section 781) primarily targets intoxicating hemp products, and non-intoxicating CBC and CBD products are expected to remain broadly legal. For the full federal context, see our Delta-8 legal states guide.
For drug testing, neither CBC nor CBD is the target of standard THC drug tests. Pure isolates (CBC isolate or CBD isolate) with certificates of analysis showing 0 detectable THC should not trigger a positive result. Full-spectrum products from either contain trace THC (up to 0.3% by dry weight) that can produce a positive test with regular use. For the full drug-test picture, read our guide on whether CBD shows up on a drug test.
Decision Framework: Which Should You Use?
Choose CBD if:
- You want the cannabinoid with the deepest evidence base and FDA validation
- Cost matters (CBD is significantly cheaper per mg)
- Your goal is anxiety, sleep, epilepsy (Rx only), or general wellness
- You want broad human safety data
- You’re new to cannabinoids and want the most-documented option
Choose CBC if:
- You’re specifically interested in TRPA1-driven pain or inflammation mechanisms
- Your use case is skin or acne (Oláh 2016 sebocyte data)
- You’re experimenting with minor cannabinoids and want the one with the most distinctive receptor pharmacology
- You’re willing to accept the “no human trials” evidence caveat
- You can afford the premium cost
Combine them if:
- Your use case is inflammation-related and you want the Grogan 2023 pattern
- You’ve tried one alone and want to layer the other
- You’re okay paying more for a combination product
Consider neither if:
- Your condition has established evidence-based medical treatments (don’t substitute CBC or CBD for proven therapies)
- You take prescription medications with significant interaction risk and haven’t talked to a doctor
- You’re in a role that drug-tests for THC and you want zero risk (stick to pure isolates with clean COAs)
Practical starting point: If you’ve never used either, start with CBD (cheaper, broader evidence, safer introduction). If CBD doesn’t address your specific concern (particularly TRPA1-associated inflammatory pain or skin applications), try CBC as the targeted second choice. Combining them makes sense for inflammation-related goals based on the Grogan 2023 finding.
Frequently Asked Questions
CBC is a potent selective TRPA1 agonist (EC50 ~90 nM) with additional CB1, CB2, and adenosine A1 activity. CBD is a negative allosteric modulator at CB1 with strong 5-HT1A agonism, TRPV1 effects, and FAAH inhibition. CBD has FDA-approved Epidiolex and extensive human research. CBC has zero human clinical trials as of April 2026 and relies on preclinical (animal and in vitro) evidence. Both are non-psychoactive.
Yes, one. Grogan et al. 2023 in Annals of Plastic Surgery tested CBC alone, CBD alone, and CBC+CBD combination in a murine collagen-induced arthritis model. The combination outperformed either compound alone in reducing paw swelling between weeks 3 and 5. This is the only published direct head-to-head comparison. It’s a small animal study, not a human trial.
Depends on the pain type. CBC’s TRPA1 mechanism is novel and may have specific advantages for TRPA1-driven inflammatory pain (Maione 2011 demonstrated this in rats). CBD has broader human pain data across more pain types including neuropathic, musculoskeletal, and inflammatory pain. For inflammation-related pain specifically, the Grogan 2023 combination approach (CBC + CBD together) outperformed either alone in the mouse arthritis model. If your pain is established and you want well-researched options, CBD is the default. If you want to target TRPA1 specifically, CBC has mechanistic appeal.
No. CBC binds the CB1 cannabinoid receptor weakly and does not produce intoxication at typical doses. Its most distinctive activity is at TRPA1 channels, which are not associated with psychoactive effects. Like CBD, CBC is categorized as non-psychoactive.
CBC is present in small amounts in mature cannabis flower (typically less than 1% of total cannabinoids). To produce commercial CBC, manufacturers either grow specialty CBC-dominant strains harvested early or chromatographically isolate CBC from concentrated extracts. Both are more expensive than extracting CBD from hemp flower that’s naturally dominant in CBD. Expect CBC to cost 3 to 8 times more per mg than equivalent CBD.
Yes. They engage different receptor systems (CBC at TRPA1, CBD at CB1 NAM + 5-HT1A + FAAH) so the combination is mechanistically reasonable. The Grogan 2023 mouse arthritis study found the combination outperformed either compound alone for swelling reduction, which is the one direct evidence for combining them. No human trial has validated the combination, but the preclinical signal supports it for inflammatory applications specifically.
Picking Between CBC and CBD
CBC vs CBD is less a contest and more a match-to-purpose decision. CBD for general wellness, evidence-backed daily use, anxiety, sleep, and epilepsy under medical care. CBC for specific TRPA1-related mechanisms, skin applications, or experimentation with minor cannabinoids at a premium cost. Both for inflammation-related goals where the Grogan 2023 combination finding applies.
Whichever direction you go, verify dose and purity via third-party certificates of analysis. TribeTokes publishes COAs on every batch. Our CBD vape cartridges are lab tested with full cannabinoid and terpene profiles.
For deeper context, our CBC benefits guide covers the full preclinical evidence on CBC. Our CBD vs THC guide covers CBD vs the psychoactive cannabinoid. Our CBG vs CBD guide covers another minor cannabinoid next to CBD. And for sleep-focused comparison, the CBN vs CBD for sleep guide covers the third common minor cannabinoid question. For the synergy science underneath all of this, our entourage effect guide covers how cannabinoid combinations work.
Lab tested. Transparent. No cannabinoid claims without a citation.
Shop TribeTokes Lab-Tested Hemp Products
Full third-party COAs on every batch. Woman-owned since 2017. Research-aligned cannabinoid dosing.