

Walk into any cannabis shop and you’ll hear the same pitch: CBN is the sleep cannabinoid, CBD is the anxiety cannabinoid, and you want both in your sleep gummy. Here’s what the clinical literature actually says. CBN has exactly one well-designed placebo-controlled trial for sleep outcomes (published in 2024), and it showed modest but real benefit at 20mg. CBD has more studies but weaker direct-sleep evidence, with most of the sleep improvement appearing to be secondary to anxiety reduction. There is no published head-to-head randomized trial comparing CBN and CBD for sleep. This guide walks through what’s actually been tested, what the results showed, what the marketing claims are really based on, and how to pick a product that matches the evidence.
🧪 Lab Tested | 👩💼 Woman-Owned | 🏆 Est. 2017
IN THIS GUIDE
- The Short Answer
- What Is CBN, Actually?
- What Is CBD, Actually?
- Where the “CBN Is the Sleep Cannabinoid” Myth Came From
- CBN for Sleep: What the Clinical Evidence Shows
- CBD for Sleep: What the Clinical Evidence Shows
- The Head-to-Head Comparison (Or Lack of One)
- The Myrcene Confounder: It Might Not Be CBN at All
- How Each Cannabinoid Interacts with Sleep Systems
- Dosing: What the Studies Used vs What’s in Your Product
- Side Effects and Drug Interactions
- A Decision Framework: Which to Try First
- How to Evaluate a Sleep Cannabinoid Product
- Frequently Asked Questions
- Shop TribeTokes
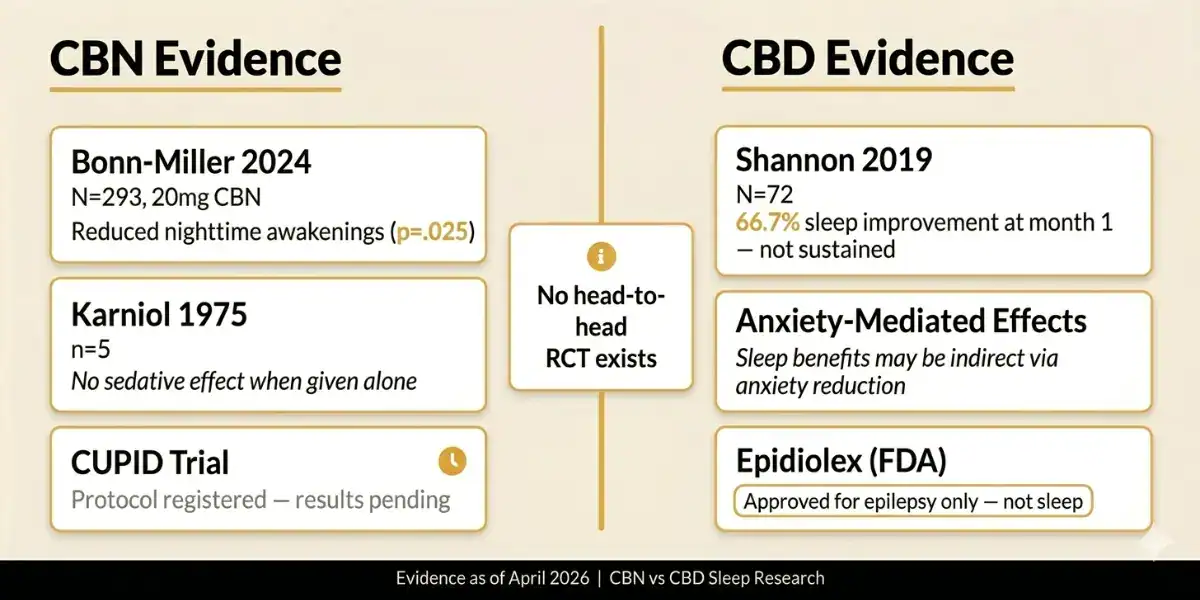
CBN vs CBD for Sleep at a Glance
| Best sleep RCT evidence | CBN. Bonn-Miller et al. 2024 (N=293) showed 20mg CBN reduced awakenings (p=.025) |
| CBD direct-sleep evidence | Shannon 2019 (N=72, open-label) showed 66.7% improved sleep in month 1, but benefits were not sustained over 3 months |
| Head-to-head CBN vs CBD trial | None published. No RCT directly compares the two for sleep outcomes |
| CBN + CBD combo | Bonn-Miller 2024 tested combinations — CBD did NOT augment CBN’s effects |
| Research-backed CBN dose | 20mg for sleep disturbance (Bonn-Miller 2024) |
| Research-backed CBD dose range | 25-175mg/day (Shannon 2019), most patients on 25mg |
| Commercial CBN products | Typically 2-5mg per dose, below researched-effective doses |
| The “indica = sleepy” confusion | Likely driven by myrcene terpene content, not CBN content |
| Primary references | Bonn-Miller 2024 (RCT), Corroon 2021 (review), Shannon 2019 (CBD case series), Karniol 1975 (historical) |
The Short Answer
If you want the research-supported answer: CBN has slightly stronger direct-sleep evidence than CBD, based on a single well-designed 2024 RCT. In that study, 20mg of CBN nightly for seven nights reduced nighttime awakenings and overall sleep disturbance compared to placebo, with no impact on daytime fatigue. CBD alone has no equivalent-quality sleep trial. Most CBD sleep research is either open-label or looks at CBD for anxiety, with sleep as a secondary outcome.
If you want the honest answer: the CBN evidence base is thin (one solid trial), the effect sizes are modest, and many commercial CBN products contain 2 to 5mg per dose, which is below the researched-effective 20mg dose. CBD may work better for anxiety-driven sleep problems specifically, even if it doesn’t act as a direct sedative. And the “indica makes you sleepy” folklore that cannabis culture attributes to CBN is probably more about terpenes (myrcene in particular) than about CBN levels.
The rest of this guide walks through every piece of that.
What Is CBN, Actually?
Cannabinol (CBN) is a cannabinoid, but unlike CBD and THC, it’s not synthesized in meaningful quantities by the cannabis plant directly. CBN is primarily a degradation product of delta-9 THC. When THC-rich cannabis is exposed to oxygen, heat, or UV light over time, the THC molecule oxidizes and converts into CBN. That’s why old, improperly stored cannabis tends to have higher CBN content than fresh flower. It’s also why commercial CBN is typically produced either by intentionally oxidizing THC or, more recently, by specialized biosynthesis and extraction.
Chemically, CBN has some overlap with THC, but CBN binds the CB1 receptor (the receptor primarily responsible for the psychoactive high) much more weakly than THC does. CBN’s binding affinity at CB1 is roughly one-tenth of THC’s. At typical doses, CBN produces only mild psychoactive effects, if any. It is sometimes described as “weakly intoxicating” rather than “non-psychoactive,” which is the more precise framing.
CBN has also been studied for antibacterial activity (against methicillin-resistant Staphylococcus aureus and other strains), anti-inflammatory effects, appetite stimulation, and its effects on bone growth. But the dominant commercial use case in 2026 is sleep, which is what this article is about.
What Is CBD, Actually?
Cannabidiol (CBD) is the most studied non-psychoactive cannabinoid in the cannabis plant. It’s the primary cannabinoid in hemp by definition (federal hemp status requires less than 0.3% delta-9 THC by dry weight, and CBD-dominant cultivars are the commercial norm). CBD does not bind the CB1 receptor the way THC does. Instead, it acts as a negative allosteric modulator at CB1 and interacts with a wide range of other receptors (5-HT1A serotonin, TRPV1 vanilloid, GPR55, PPAR-gamma, and others), which is why its pharmacology is so complex.
CBD has one FDA-approved prescription form: Epidiolex, a purified plant-derived oral solution approved in 2018 for seizures associated with Dravet syndrome, Lennox-Gastaut syndrome, and tuberous sclerosis complex. For sleep specifically, CBD is not FDA-approved and is sold as a dietary supplement or hemp product, not a medication.
For the broader CBD picture, including the difference between full spectrum, broad spectrum, and isolate, read our CBD spectrum comparison guide. For the compound-level comparison with THC, see our CBD vs THC guide.
Where the “CBN Is the Sleep Cannabinoid” Myth Came From
The story of CBN as “the sedating cannabinoid” is one of the more interesting cases of cannabis marketing outpacing actual data. The most-often cited origin is a claim from Steep Hill Labs in the 2010s that CBN was “the most sedating cannabinoid,” reportedly stating that 5mg of CBN was equivalent to 10mg of diazepam. That claim spread widely through cannabis publications and product marketing, but it was never published in a peer-reviewed paper with supporting data.
The underlying research people reach for is Karniol et al. 1975 (European Journal of Pharmacology, PMID 1221432), which tested delta-9 THC and CBN in five male volunteers. Participants reported feeling drugged, drunk, dizzy, and drowsy under the THC condition, but not under the CBN condition. When CBN and THC were combined, reported effects were additive beyond THC alone. So Karniol 1975 is actually evidence that CBN alone doesn’t produce sedation in humans. The combination might have mattered, but CBN alone did not.
The 2021 review that most thoroughly unpacked this is Jamie Corroon’s “Cannabinol and Sleep: Separating Fact from Fiction” in Cannabis and Cannabinoid Research (2021, PMID 34468204). Corroon concluded that at the time of the review, there was insufficient clinical evidence to support CBN’s sleep-promoting effects. Specifically: no published clinical trials using validated sleep questionnaires or polysomnography, most human research dating from the 1970s-1980s with tiny homogeneous samples, and commercial products typically containing 5mg or less of CBN, far below any researched-effective dose.
Corroon’s review was published in 2021. The first well-designed placebo-controlled CBN sleep trial wasn’t published until 2024. That’s the trial that reshapes the picture.
CBN for Sleep: What the Clinical Evidence Shows
As of April 2026, the single strongest piece of clinical evidence for CBN and sleep is Bonn-Miller et al. 2024, published in Experimental & Clinical Psychopharmacology (PMID 37796540, DOI 10.1037/pha0000682). This is the first modern, adequately powered, placebo-controlled randomized trial to specifically test CBN on sleep quality.
Study design
- Double-blind, randomized, placebo-controlled
- N = 293 adults (modified intent-to-treat analysis)
- Five conditions: placebo, 20mg CBN alone, 20mg CBN + 10mg CBD, 20mg CBN + 20mg CBD, 20mg CBN + 100mg CBD
- Treatment duration: seven consecutive nights
- Primary outcome: sleep quality
Key findings
- 20mg CBN vs placebo: Trend toward improved sleep quality (odds ratio 2.26, p = .082; not statistically significant at conventional thresholds but directionally positive)
- Nighttime awakenings: Significantly reduced on CBN (p = .025)
- Overall sleep disturbance: Significantly reduced on CBN (p = .023)
- Daytime fatigue: No impact. This is important: the sleep benefit did not come with a next-day drowsiness penalty
- CBD addition: Adding 10mg, 20mg, or even 100mg of CBD to the 20mg CBN did not positively augment the CBN effects
The CBD-addition finding is the most commercially inconvenient result in the paper. Sleep products marketed as “CBN + CBD work better together” don’t have support from the one RCT that tested the combination. The paper shows CBN alone at 20mg producing the sleep benefit, and CBD at three different doses not adding to it.
Beyond Bonn-Miller 2024, additional CBN sleep research includes:
- The CUPID trial protocol (PMC10450062), a more recent randomized double-blind placebo-controlled crossover study testing 30mg and 300mg CBN in insomnia disorder. This is a proof-of-concept trial, with results anticipated but not yet fully published
- Preclinical rat data (2024, Neuropsychopharmacology) showed that CBN and its active metabolite influenced sleep architecture, increasing both NREM and REM sleep in rats, with biphasic effects at different doses
Taken together: CBN has moved from “mostly folklore” in 2021 to “one solid RCT showing modest benefit at 20mg” in 2024. The evidence base is still thin relative to, say, benzodiazepines or Z-drugs, but it’s no longer mythology.
CBD for Sleep: What the Clinical Evidence Shows
CBD has more total research than CBN, but less direct-sleep research than you might expect. The most cited study specific to sleep is Shannon et al. 2019, “Cannabidiol in Anxiety and Sleep: A Large Case Series” in The Permanente Journal (PMID 30624194).
Study design
- Retrospective chart review (open-label, no control group, no randomization)
- N = 72 adults at a psychiatric clinic (47 with anxiety as primary complaint, 25 with sleep as primary complaint)
- Dose: starting 25mg/day in capsule form. Range 25 to 175mg/day. Most patients remained at 25mg
- Duration: three months with monthly assessments
- Sleep measure: Pittsburgh Sleep Quality Index (PSQI), a validated 19-item self-report instrument
Key findings
- Anxiety scores decreased within the first month in 57 of 72 patients (79.2%) and remained decreased
- Sleep scores improved within the first month in 48 patients (66.7%) but “fluctuated over time”
- Authors’ overall conclusion: “Sleep scores displayed no sustained improvements during the 3-month study”
- Tolerability: CBD was well tolerated in all but three patients
The Shannon study is important historically because it put CBD sleep benefits on the map for a lot of clinicians and consumers. But it has serious methodological limitations that the authors acknowledged: no control group, open-label design (patients knew they were taking CBD), concurrent psychiatric medications that confounded attribution, a younger-than-typical sample, and the likelihood of inflated placebo effects given cannabis’s reputation. It’s a hypothesis-generating study, not a confirmatory one.
The larger pattern in CBD sleep research is that CBD’s sleep effects appear to be indirect, mediated largely through anxiety reduction. People who fall asleep more easily and stay asleep longer on CBD often do so because their anxiety level is lower, not because CBD is a direct sedative. That’s why CBD tends to work better for people whose sleep problem is downstream of anxiety, and less well for people with primary insomnia unrelated to anxiety.
The National Center for Complementary and Integrative Health (NCCIH) maintains a cautious summary of the state of cannabinoid research for sleep, which is worth reading if you want the government-authoritative view on what the evidence does and doesn’t support.
The Head-to-Head Comparison (Or Lack of One)
Here’s the honest gap in the research: no published randomized controlled trial has directly compared CBN and CBD as sleep interventions. The closest thing we have is Bonn-Miller 2024, which tested CBN alone against CBN+CBD combinations against placebo. But it did not include a CBD-alone condition. You can infer that CBD alone would perform similarly to placebo in that trial’s framework, since adding CBD to CBN didn’t augment the effect. But that’s inference, not direct comparison.
What this means practically: any claim that “CBN is better than CBD for sleep” or “CBD is better than CBN for sleep” is a conclusion drawn from indirect comparisons across different studies with different designs, populations, and outcome measures. It’s not a claim backed by head-to-head RCT data.
The indirect comparison we can make, cautiously:
- CBN 20mg has one RCT showing modest sleep-specific benefit (reduced awakenings, reduced sleep disturbance)
- CBD 25mg in Shannon 2019 showed early sleep improvement that was not sustained, in an uncontrolled design
- CBD appears to work better as an anxiety intervention that secondarily improves sleep, not as a direct sleep agent
- Commercial products combining CBN + CBD + melatonin have mixed evidence; Bonn-Miller 2024 specifically found that adding low-dose CBN and CBC to a melatonin formulation did not significantly augment a 5mg melatonin effect
The Myrcene Confounder: It Might Not Be CBN at All
If you’ve ever heard that “indica strains are sedating because of CBN,” that folk claim has a factual problem. Fresh, well-stored cannabis flower typically contains only trace amounts of CBN, usually under 1% of total cannabinoid content and often much less. The dominant cannabinoid in most indica strains is THC, not CBN. So the CBN content can’t realistically explain the sedating character that some strains reliably produce.
A more defensible explanation is the terpene profile, particularly myrcene. Myrcene is a common monoterpene in cannabis, and strains sometimes called “couch-lock” tend to be higher in myrcene. Myrcene has been studied in animal models for sedative and muscle relaxant effects, and it’s been proposed as the actual driver of the “indica relaxation” phenomenon. Ethan Russo’s 2011 review in the British Journal of Pharmacology (“Taming THC”) laid out the case for terpene-cannabinoid synergy in detail and specifically discussed myrcene’s sedative-adjacent effects.
The practical takeaway: if a gummy says “contains indica-style CBN for sleep,” be skeptical that CBN is doing the work. The sedating effect is more likely coming from the combination of any THC present, myrcene or linalool content, and in CBN-specific products, sometimes doses high enough (like the 20mg from Bonn-Miller 2024) to produce a genuine pharmacological effect. A 2mg CBN gummy marketed as a sleep aid is below any researched-effective dose and is likely riding on folklore rather than pharmacology.
For a deeper dive on terpenes and how they shape cannabis effects, our terpenes guide breaks down myrcene, linalool, beta-caryophyllene, and the others. And for the underlying science on cannabinoid-terpene synergy, the entourage effect guide covers the mechanisms.
How Each Cannabinoid Interacts with Sleep Systems
Why might CBN and CBD affect sleep at all? The mechanisms are partially overlapping and partially distinct.
CBN and sleep mechanisms
CBN binds the CB1 cannabinoid receptor as a partial agonist, though with roughly one-tenth the affinity of THC. CB1 activation in the central nervous system is associated with reduced neuronal excitability, dampening of stress responses, and altered sleep architecture (typically increased NREM sleep in animal studies). CBN also interacts with TRPV2 and TRPA1 channels, and may have effects on GABAergic signaling, though the human data here is sparse. The proposed mechanism for CBN’s sleep effect is a combination of mild CB1 agonism and other endocannabinoid-adjacent pathways that dampen the activity patterns associated with frequent awakenings.
CBD and sleep mechanisms
CBD does not bind CB1 directly. Instead, it’s a negative allosteric modulator of CB1, reducing the effect of whatever else is binding to the receptor. CBD’s sleep-relevant mechanisms are thought to include:
- 5-HT1A serotonin receptor agonism, contributing to anxiety reduction, which secondarily improves sleep
- FAAH enzyme inhibition, slowing the breakdown of anandamide (your body’s own endocannabinoid), which may produce CB1-adjacent effects without direct binding
- TRPV1 receptor desensitization, with downstream effects on pain and inflammatory signaling that can affect sleep quality in people with pain-related sleep disruption
- Possible adenosine reuptake inhibition, with effects similar to the mechanism by which caffeine’s reverse is a driver of sleep drive
The contrast matters clinically. CBN appears to have a more direct effect on sleep itself. CBD appears to have a more downstream effect on sleep by reducing anxiety and hyperarousal. Two different pharmacological profiles, two different use cases.
Dosing: What the Studies Used vs What’s in Your Product
This is the section where commercial CBN products fall apart. The research-effective doses and the commercial doses are not the same.
| Compound | Research Dose (per study) | Typical Commercial Dose | Gap |
|---|---|---|---|
| CBN | 20mg nightly (Bonn-Miller 2024) | 2 to 5mg per gummy | Commercial dose is 4-10x below the researched-effective dose |
| CBD (sleep) | 25mg/day (most patients in Shannon 2019) | 10 to 50mg per gummy or serving | Commercial dosing is roughly aligned with the low end of research |
| CBD (anxiety-driven sleep) | 25 to 75mg/day (Shannon 2019 subset) | Requires 2-3 gummies to reach | Usually achievable with commercial products if dosed higher |
The practical implication: if you take a “sleep gummy” with 3mg CBN and 10mg CBD and feel nothing, you haven’t proven that cannabinoids don’t work for your sleep. You’ve proven that below-research doses don’t work for your sleep. A 20mg CBN dose (the Bonn-Miller amount) would require taking 6 to 10 standard gummies, which is impractical and often expensive.
For CBN specifically, look for products dosed at 15mg or higher per serving if you want to approach research-backed dosing. Some brands now market 25mg and 50mg CBN products in response to the Bonn-Miller data. For CBD, 25mg+ per dose is reasonable for general sleep support; higher doses (50 to 100mg) may be more appropriate for anxiety-driven sleep problems.
Side Effects and Drug Interactions
Both CBN and CBD have relatively mild side effect profiles, but there are differences worth knowing.
CBN
- Mild drowsiness (the point of using it, but can carry into next-day if dosed too late or too high)
- Possible trace psychoactivity at high doses (since CBN binds CB1 weakly)
- Dry mouth is occasionally reported
- Drug interaction potential with CYP450 substrates, though less studied than CBD
- Bonn-Miller 2024 reported no significant adverse event differences between CBN and placebo at 20mg
CBD
- Drowsiness at higher doses
- Diarrhea at higher doses (more common in clinical trials using 200+ mg/day)
- Fatigue and decreased appetite in a subset of users
- Drug interactions are the bigger concern. CBD inhibits cytochrome P450 enzymes (CYP3A4 and CYP2C9 specifically), which metabolize a wide range of prescription medications including blood thinners, anti-seizure drugs, immunosuppressants, and certain antidepressants and heart medications. If you take prescription medication, ask your doctor or pharmacist before starting CBD
- The WHO Expert Committee on Drug Dependence concluded in 2018 that pure CBD has a good safety profile and no abuse potential
Drug test consideration
Full-spectrum CBN and CBD products may contain trace delta-9 THC (up to 0.3% by dry weight under federal hemp law), which can trigger a positive workplace drug test with regular use. Pure CBN isolate and CBD isolate with verified certificates of analysis showing zero detectable THC are the lower-risk options. For the full breakdown, see our guide on whether CBD shows up on a drug test.
A Decision Framework: Which to Try First
If you’re starting from scratch and want a research-informed path forward:
Consider CBN first if:
- Your main sleep complaint is frequent nighttime awakenings or fragmented sleep (what Bonn-Miller 2024 specifically measured improvement on)
- Your anxiety is relatively low and not driving your insomnia
- You can find a product at 15mg+ CBN per serving (the commercial-reality matching to research-dose)
- You want something that doesn’t affect next-day fatigue
- You’ve already tried sleep hygiene basics and OTC options without success
Consider CBD first if:
- Your sleep problem clearly ties to anxiety or rumination at bedtime
- You want a non-intoxicating option with a broader safety profile
- You can commit to at least 25mg/day as a starting dose, with potential titration to 50 to 75mg
- You’re not on medications with CYP3A4/CYP2C9 interaction risk (or have talked to a doctor about it)
- You’ve tried CBN at research-effective doses and didn’t find it useful
Consider combining them (or trying in sequence) if:
- You’ve tried one alone without success and want to layer
- Note that Bonn-Miller 2024 did not find that CBD added to CBN. That doesn’t mean combinations can’t work for you individually, just that the combination didn’t outperform CBN alone on average
- A combined product with both at research-effective doses (say, 20mg CBN + 25mg CBD) is a reasonable experiment if single-compound products haven’t worked
Consider not using cannabinoids at all if:
- Your sleep problem is mild and responds to sleep hygiene changes (consistent bedtime, cool dark room, no screens before bed, limiting evening caffeine and alcohol)
- You have chronic insomnia that meets clinical criteria: evidence-based treatments like cognitive behavioral therapy for insomnia (CBT-I) have stronger data than any cannabinoid
- You’re on medications with significant interaction risk and your doctor hasn’t approved adding cannabinoids
- You’re drug tested for work or legal reasons and the risk of a positive result outweighs potential benefit
The honest starting point: before any cannabinoid, optimize sleep hygiene and consider CBT-I if the problem is chronic. Cannabinoids are supplementary tools, not first-line interventions. The evidence base for both CBN and CBD is modest, and the biggest returns in sleep tend to come from behavioral changes that don’t require any product.
How to Evaluate a Sleep Cannabinoid Product
Once you’ve decided a cannabinoid sleep product is worth trying, the product-selection criteria are the same as any other cannabinoid purchase, with a few sleep-specific additions.
- Check the actual dose. Not the total bottle content, the per-serving dose. For CBN, aim for 15 to 25mg per serving. For CBD sleep support, 25 to 50mg per serving
- Verify the certificate of analysis. A legitimate brand publishes third-party lab reports for every batch, showing cannabinoid potency, absence of pesticides, heavy metals, residual solvents, and microbial contamination. Our guide on reading certificates of analysis walks through what to look for
- Check the THC content. If you’re drug tested, look for CBN isolate or CBD isolate products with 0 detectable THC. Full-spectrum and broad-spectrum products carry more risk
- Match the delivery method to your sleep issue. For trouble falling asleep, faster-acting forms (sublingual tinctures) make sense. For staying asleep, longer-acting forms (gummies or capsules) are more useful. For the bioavailability tradeoffs by method, see our CBD bioavailability guide
- Ignore “entourage effect” marketing unless specific. A product saying “entourage effect supports better sleep” without naming specific terpenes or cannabinoids is selling vibes. A product naming myrcene content in mg, or disclosing the full cannabinoid profile with quantities, is being transparent
- Beware melatonin stacking. Some “sleep” products contain melatonin at 5 to 10mg alongside cannabinoids. Melatonin works best at much lower doses (0.3 to 1mg) and can cause next-day grogginess at higher doses. If you want to test cannabinoids for sleep, isolate the variable and avoid combination products initially
- Start low and observe over a week. Don’t judge a cannabinoid sleep product on one night. Sleep benefit, when it happens, tends to show up over 3 to 7 nights of consistent use
Frequently Asked Questions
Based on the current clinical evidence, CBN has slightly stronger direct-sleep data. Bonn-Miller et al. 2024 (Experimental & Clinical Psychopharmacology, N=293) showed 20mg CBN nightly reduced awakenings and overall sleep disturbance compared to placebo. CBD has more total research but less direct-sleep evidence; most CBD sleep benefit appears to come from anxiety reduction. There is no published randomized trial that directly compares CBN vs CBD head-to-head for sleep.
The research-effective dose from Bonn-Miller 2024 was 20mg nightly, taken for at least seven consecutive nights. Many commercial CBN sleep products contain only 2 to 5mg per serving, well below this amount. If you want to approach the researched-effective dose, look for products at 15 to 25mg CBN per serving. Start at the lower end and observe over a week before adjusting.
In Bonn-Miller et al. 2024, CBN at 20mg did not produce significant next-day fatigue compared to placebo. That’s consistent with CBN’s relatively weak activity at the CB1 receptor. Individual responses vary, and higher doses or late-night timing could produce next-day effects in some people. If you experience residual drowsiness, try dosing earlier in the evening or reducing the amount.
Historically, CBN was expensive to produce at commercial scale, and most sleep-marketing products were built on the “most sedating cannabinoid” claim rather than on researched-effective doses. Products with 2 to 5mg per serving were economical to manufacture and relied on consumer expectations rather than pharmacology. Now that Bonn-Miller 2024 has established a 20mg reference dose, newer products are increasingly dosed in the 15 to 25mg range. Check the per-serving amount on the label, not the total bottle content.
Mostly not. Fresh cannabis flower typically contains less than 1% CBN total, which isn’t enough to explain the sedating effect of specific strains. The more likely explanation is the terpene profile, particularly myrcene content, combined with the total THC and other cannabinoid levels. “Couch-lock” strains tend to be higher in myrcene, and myrcene has been studied in animal models for sedative-adjacent effects. Ethan Russo’s 2011 review on cannabinoid-terpene synergy lays out the case in detail.
You can, and some commercial products combine them. But Bonn-Miller 2024 specifically tested 20mg CBN with 10mg, 20mg, and 100mg of added CBD, and the CBD addition did not augment the CBN sleep effects. That doesn’t mean combinations can’t help any individual. It means the group-average data from the best RCT available doesn’t support the common “CBN + CBD work better together” marketing claim for sleep specifically.
Shopping for the Evidence-Based Product
Picking a CBN or CBD sleep product is mostly an exercise in reading labels and COAs carefully. The research-supported dose for CBN is 20mg; the research-supported starting dose for CBD is 25mg. Anything significantly below those numbers is priced on marketing rather than pharmacology.
TribeTokes publishes third-party certificates of analysis for every batch, with full cannabinoid and terpene profiles so you know exactly what you’re getting per serving. Our CBD vape cartridges and companion CBD products are dosed at measurable, research-informed amounts. For the parallel science on the compound-level differences, our CBD vs THC guide breaks down the pharmacology. For format choice (full spectrum vs broad spectrum vs isolate), our spectrum comparison guide covers the decision.
Lab tested. Transparent. No sleep promises we can’t back with a citation.
Shop TribeTokes Lab-Tested CBD and THCa
Full third-party COAs on every batch. Woman-owned since 2017. Research-informed dosing on transparent products.