

CBG and CBD are both non-psychoactive cannabinoids produced by the same cannabis plant, and they get treated as if they’re basically the same thing. They’re not. CBG is the chemical precursor the plant starts with (that’s why it’s called the “mother cannabinoid”), and CBD is one of the compounds the plant converts it into. They hit different receptors, have wildly different clinical evidence bases (CBD has FDA-approved Epidiolex plus decades of study, CBG has one human trial from 2024), and they cost very different amounts to produce. This guide runs the complete side-by-side comparison: chemistry, pharmacology, clinical evidence, dosing, drug tests, cost, and how to decide which one fits your actual situation.
🧪 Lab Tested | 👩💼 Woman-Owned | 🏆 Est. 2017
CBG vs CBD at a Glance
| Psychoactive? | Neither. Both non-intoxicating at typical doses |
| Role in the plant | CBG is the precursor (“mother cannabinoid”). CBD is a downstream product |
| Plant abundance | CBD: dominant in hemp. CBG: typically <1% in mature flower |
| CB1 interaction | CBG: weak partial agonist. CBD: negative allosteric modulator (Laprairie 2015) |
| Distinctive receptor | CBG: α-2 adrenoceptor. CBD: 5-HT1A + FAAH inhibition |
| Human clinical trials | CBG: 1 RCT (Cuttler 2024, N=34). CBD: dozens of RCTs plus FDA-approved Epidiolex |
| FDA-approved drug | CBG: none. CBD: Epidiolex (2018, epilepsy) |
| Research-dose anxiety benefit | CBG: 20mg (Cuttler 2024). CBD: 25-75mg typical range |
| Cost per mg | CBD: cheapest mass-market cannabinoid. CBG: 2-5x more expensive |
| Drug test risk | Both low for verified isolates. Both moderate for full-spectrum |
| Direct head-to-head RCT | None published as of April 2026 |
The Short Answer
If you want the one-paragraph version: CBD is the more studied, more available, and cheaper cannabinoid with broad general-purpose use cases. CBG is the newer, pricier, and less-studied cannabinoid with emerging evidence specifically for anxiety and focus, backed by a single high-quality 2024 human trial. They have overlapping but distinct pharmacology. CBD binds the CB1 cannabinoid receptor as a negative allosteric modulator and engages serotonin and TRPV1 systems. CBG is a partial agonist at CB1/CB2 and engages α-2 adrenergic receptors that are involved in focus and attention. CBD has one FDA-approved prescription form (Epidiolex, for epilepsy). CBG has none. Neither gets you high.
Practically: if you want a well-characterized cannabinoid at a reasonable price for general wellness or anxiety management, CBD is the default. If you specifically want the “focus and clear-headed calm” profile that the first human CBG trial documented, and you’re willing to pay more for a less-tested compound, CBG is worth trying. The rest of this guide walks through why those conclusions hold up and where the nuances matter.
What Is CBG?
Cannabigerol (CBG) is a cannabinoid produced by the cannabis plant, but unlike THC or CBD, it’s present in very small amounts in mature flower. That’s because the plant uses CBG’s acidic form (CBGA) as a chemical precursor and converts most of it into the acidic forms of THC, CBD, and CBC as it matures. By the time most cannabis flower is harvested, CBG content is usually below 1% of total cannabinoids, which is why the compound is sometimes called the “mother cannabinoid.”
CBG is not psychoactive at typical doses. It binds the CB1 cannabinoid receptor (the one responsible for THC’s high) weakly, and it doesn’t produce euphoria or altered perception. Its more distinctive pharmacology lives elsewhere: at α-2 adrenergic receptors, serotonin 5-HT1A receptors, and as an inhibitor of anandamide reuptake. The 2021 pharmacology review by Nachnani, Raup-Konsavage, and Vrana in the Journal of Pharmacology and Experimental Therapeutics (volume 376, issue 2, pages 204-212) laid out these mechanisms in detail.
For the full benefits picture on CBG specifically, including the 2024 human anxiety trial and the preclinical work on IBD, MRSA, and Huntington’s disease, read our CBG benefits guide.
What Is CBD?
Cannabidiol (CBD) is the most studied non-psychoactive cannabinoid in cannabis. It’s the dominant cannabinoid in hemp by design: federal hemp status requires less than 0.3% delta-9 THC by dry weight, and CBD-dominant cultivars are what most commercial hemp production targets. CBD research has a decade-plus head start on CBG, with thousands of papers, multiple systematic reviews, and one FDA-approved prescription drug.
CBD’s pharmacology is multi-target. Unlike THC, it doesn’t bind the CB1 active site. Instead, a 2015 study by Laprairie and colleagues in the British Journal of Pharmacology (PMID 26218440) showed CBD acts as a negative allosteric modulator at CB1, binding a different site on the receptor and reducing how strongly other ligands (including THC) activate it. CBD also agonizes 5-HT1A serotonin receptors, interacts with TRPV1 and GPR55, and inhibits the FAAH enzyme that breaks down anandamide.
CBD has one FDA-approved prescription form: Epidiolex, approved in 2018 for seizures associated with Dravet syndrome, Lennox-Gastaut syndrome, and tuberous sclerosis complex. It’s the only FDA-approved plant-derived cannabis drug. For the full CBD context including the compound-level comparison with THC, see our CBD vs THC guide.
The Chemistry: Same Plant, Different Molecules, Biosynthetic Relationship
CBG and CBD come from the same source, but their relationship is chronological rather than parallel. Here’s how it works in the growing plant.
The cannabis plant first synthesizes CBGA (cannabigerolic acid), the acidic precursor to all major cannabinoids. As the plant matures, specialized enzymes act on CBGA and convert it into three different acidic cannabinoids: THCA (which becomes THC when heated), CBDA (which becomes CBD), and CBCA (which becomes CBC). Whatever CBGA doesn’t get converted remains as CBGA, which decarboxylates with heat or age to become CBG.
So when you see a product labeled “CBG,” you’re looking at either:
- A compound from a strain bred to retain more CBGA (typically by harvesting early before much conversion has happened, or by using genetics with lower enzyme activity for the downstream conversions)
- A compound extracted from plant material where CBG has been chromatographically isolated
- A compound produced via biosynthesis (not from whole plant material at all)
The fact that CBG is the starting material means mature flower typically contains very little CBG. Most commercial CBG products use concentrated extracts or specialty “CBG-dominant” strains. CBD, by contrast, is the dominant finished product of the plant’s biosynthesis and is abundant in mature hemp flower, which is part of why CBD is so much cheaper to produce.
Both CBG and CBD share the molecular formula pattern of the cannabinoid family: they’re polyphenolic compounds with alkyl side chains and no nitrogen. They differ in the specific ring structures. CBG has an uncyclized central structure that gives it its characteristic flexible pharmacology. CBD has a closed-ring structure at one end but an open ring at the other (the feature that prevents it from activating CB1 like THC does).
Receptor Pharmacology Side-by-Side
This is where CBG and CBD look most different. They overlap on some receptor systems but have distinct primary mechanisms.
| Receptor / Enzyme | CBG Activity | CBD Activity |
|---|---|---|
| CB1 cannabinoid receptor | Weak partial agonist | Negative allosteric modulator (Laprairie 2015) |
| CB2 cannabinoid receptor | Partial agonist | Indirect activity, less characterized |
| α-2 adrenoceptor | Partial agonist (Nachnani 2021) | Minimal direct activity |
| 5-HT1A serotonin | Active (Nachnani 2021) | Agonist (established) |
| TRPV1 | Moderate activity | Agonist / desensitizer |
| FAAH inhibition | Weak | Notable (raises anandamide levels) |
| PPAR-gamma | Active | Active |
| GPR55 | Less-characterized | Active (complex effects) |
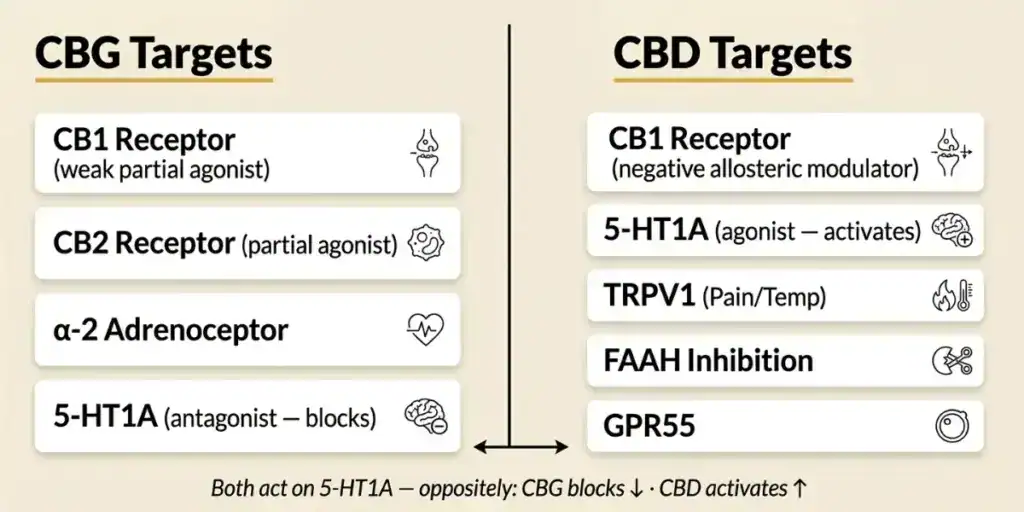
The key takeaway: CBG engages α-2 adrenergic receptors in ways CBD doesn’t. Alpha-2 agonists (like the prescription drugs guanfacine and clonidine) are used clinically for attention support, and this mechanism is a plausible basis for the “focus” profile that CBG users describe. CBD’s distinctive mechanism is the 5-HT1A-plus-FAAH-plus-TRPV1 combination, which is a plausible basis for its anxiety-reducing, mood-modulating effects.
For the underlying framework on cannabinoid receptor pharmacology more broadly, our entourage effect guide covers how cannabinoid-terpene interactions at receptor systems produce the combined effects of full-plant extracts.
Clinical Evidence: CBD’s Depth vs CBG’s Recency
The clinical evidence comparison is lopsided, and it’s worth being honest about.
CBD’s evidence base
- FDA-approved medication: Epidiolex (plant-derived CBD) is approved for three rare pediatric epilepsy syndromes. Approval required multiple randomized controlled trials with placebo comparison
- Anxiety and sleep: The widely cited Shannon et al. 2019 case series in The Permanente Journal (PMID 30624194, N=72) showed anxiety reduction in 79.2% of patients and sleep improvement in 66.7% in the first month at 25-175mg/day doses, though with an open-label design
- Pharmacokinetics: The Millar et al. 2018 systematic review in Frontiers in Pharmacology analyzed 24 human pharmacokinetic studies
- Safety: The WHO Expert Committee on Drug Dependence concluded in 2018 that pure CBD has a favorable safety profile and no abuse potential
- Thousands of additional animal and human studies across pain, inflammation, neuroprotection, and psychiatric applications
CBG’s evidence base
- One human clinical trial: Cuttler et al. 2024, “Acute effects of cannabigerol on anxiety, stress, and mood,” in Scientific Reports (PMID 39003387). N=34 adults, 20mg hemp-derived CBG vs placebo, double-blind, placebo-controlled crossover. Findings: 26.5% reduction in anxiety ratings vs placebo at 20, 45, and 60 minutes post-dose. Verbal memory enhancement. No subjective drug effects, no cognitive impairment
- Animal and cell research: Multiple preclinical findings for inflammation, IBD (Borrelli 2013), antibacterial activity (Appendino 2008), neuroprotection in Huntington’s models (Valdeolivas 2015)
- Pharmacology review: Nachnani et al. 2021 (cited above) is the modern reference
- No FDA-approved drug
- No multi-trial meta-analyses
The practical implication: if you’re picking a cannabinoid based on depth of research, CBD wins by a significant margin. If you’re picking based on specific-to-anxiety acute data at a low dose, CBG’s 2024 trial is a meaningfully strong standalone data point. Most consumers shouldn’t read this as “CBD is better” but rather as “CBD is better-characterized,” which is a different claim.
Anxiety Head-to-Head
Anxiety is the use case where CBG’s evidence comes closest to rivaling CBD’s, which is surprising given how recent the CBG data is.
CBD for anxiety
The CBD evidence for anxiety is broader but mixed in quality. Shannon 2019 showed 79.2% of patients improved on anxiety scores in the first month, and anxiety improvements were sustained across three months. However, that study had no control group, no randomization, and acknowledged potential for inflated placebo effects. Smaller placebo-controlled trials have shown acute anxiety-reduction effects of CBD, often at doses in the 300-600mg range for a single acute challenge (public speaking tests, for example), and lower doses (25-50mg) in some daily-use studies.
CBG for anxiety
Cuttler 2024 is the highest-quality CBG anxiety data we have. The trial was double-blind, placebo-controlled, with a crossover design (each participant serving as their own control). 20mg hemp-derived CBG produced a 26.5% reduction in anxiety at 20, 45, and 60 minutes after ingestion compared to placebo. The effect was acute and measurable. No intoxication.
The honest comparison
On study design quality, Cuttler 2024 beats Shannon 2019 (it was randomized and placebo-controlled; Shannon was neither). On sample size, Shannon had more participants (72 vs 34). On duration, Shannon was three months; Cuttler was acute. And on dose requirements, CBG produced benefit at 20mg while CBD often requires 25mg-plus to hundreds of mg for analogous acute effects.
If anxiety is your primary goal and you want the best-designed single study at the lowest effective dose, CBG at 20mg has a claim. If you want the broader evidence base plus long-duration data, CBD has a claim. Both are defensible choices.
Focus and Memory
This is where CBG has an edge in the current evidence. The same Cuttler 2024 trial that measured anxiety also found that 20mg CBG enhanced verbal memory recall compared to placebo, with no cognitive or motor impairment. That was a secondary but statistically meaningful finding.
The mechanism is plausibly tied to CBG’s α-2 adrenoceptor activity. α-2 agonists like guanfacine are used clinically for attention and focus support. That receptor engagement is what differentiates CBG’s pharmacology from CBD’s.
CBD, by contrast, does not have published evidence supporting pro-cognitive effects at standard doses. Some studies at high doses (800mg+) have shown working memory benefits, but the effective doses are impractical for routine use and the signal is weaker than CBG’s at 20mg.
For focus specifically, CBG has better evidence at a more practical dose. If cognitive support is your priority, CBG is the more defensible pick.
Inflammation and Gut Health
Both cannabinoids have preclinical anti-inflammatory data. Borrelli et al. 2013 in Biochemical Pharmacology showed CBG reduced colitis severity in mice (DNBS model), normalized inflammatory cytokines, and reduced iNOS and myeloperoxidase activity. CBD has a parallel body of evidence including similar colitis findings and broader data on arthritis, neuroinflammation, and inflammatory skin conditions.
For general inflammation, CBD has the larger evidence base and more available consumer products dosed for that use case. For gut-specific inflammation (IBD, Crohn’s, ulcerative colitis), both cannabinoids have been studied in animal models, with CBG’s gut-focused mechanism involving CB2 receptor activity in gut immune cells being particularly studied.
Honest caveat: all of this is preclinical. No randomized human trial has established either cannabinoid as a validated treatment for IBD. If you have diagnosed inflammatory bowel disease, cannabinoid supplementation is not a substitute for medical treatment and should be discussed with a gastroenterologist, not self-administered.
Sleep
Sleep evidence favors CBD over CBG, mostly because CBG hasn’t been tested for sleep outcomes specifically. CBD’s sleep data is mixed (Shannon 2019 showed initial improvement that “fluctuated over time” rather than sustained benefit), but it exists. CBG sleep evidence is effectively absent, aside from anecdotal reports.
If sleep is your primary goal and you want a cannabinoid with at least some direct-sleep clinical evidence, CBN (cannabinol) has the strongest single RCT finding. For the CBN vs CBD comparison specifically, read our CBN vs CBD for sleep guide.
Epilepsy (CBD Only)
Epilepsy is CBD’s strongest clinical use case by a wide margin. Epidiolex (plant-derived CBD) was FDA-approved in 2018 for Dravet syndrome and Lennox-Gastaut syndrome, later expanded to tuberous sclerosis complex. The approval rested on multiple placebo-controlled randomized trials showing significant seizure reduction at prescription doses (typically 5-20 mg/kg/day, which is far higher than consumer CBD doses).
CBG has no parallel evidence for epilepsy. Preclinical work has explored related effects, but no human trial of CBG for seizure outcomes has been published. If you’re considering cannabinoid-based treatment for a seizure disorder, that’s a clinical conversation with a neurologist, and the relevant agent is Epidiolex, not CBG.
Can You Take CBG and CBD Together?
Yes, and there’s one pilot study that specifically combined them. A 2023 randomized pilot study tested a CBD + CBG beverage powder for recovery from delayed onset muscle soreness (DOMS), showing acceptable safety and tolerability across repeated dosing, though it was a small proof-of-concept rather than a definitive efficacy trial.
Mechanistically, CBG and CBD engage different but overlapping receptor systems. Taking them together could produce complementary effects: CBD’s FAAH inhibition and TRPV1 effects plus CBG’s α-2 adrenergic and CB1/CB2 partial agonism. Whether this combination outperforms either compound alone on specific outcomes hasn’t been tested in controlled human trials beyond the pilot DOMS study.
Worth noting: the Cuttler 2024 CBG anxiety trial did not test combinations with CBD. And the 2024 CBN sleep trial by Bonn-Miller found that adding CBD to CBN did not augment CBN’s sleep effects. That’s not direct evidence against CBG+CBD combinations, but it’s a cautionary data point for assuming that “more cannabinoids = more benefit.”
The practical conclusion: CBG and CBD can safely be combined, but evidence for synergy is limited. If you want to test the combination, start with one first, get a feel for how it affects you, then add the other.
Dosing: What the Studies Actually Used
| Use Case | CBG Research Dose | CBD Research Dose |
|---|---|---|
| Acute anxiety | 20mg oral (Cuttler 2024) | 25-600mg depending on study |
| Daily anxiety/sleep | Not established | 25-175mg/day (Shannon 2019) |
| Epilepsy (Rx only) | Not applicable | 5-20 mg/kg/day (Epidiolex) |
| Inflammation | Not established in humans | 25-100mg/day (varies) |
Practical dosing notes:
- Start at the low end of any range and titrate up based on response. Give a new cannabinoid at least a week of consistent use before evaluating effects
- Both CBG and CBD are lipophilic. Taking with a small fatty snack improves absorption
- Commercial CBG products often contain 5-10mg per serving, below the researched-effective 20mg anxiety dose. Check per-serving doses carefully
- For bioavailability differences by delivery method (which apply to both CBG and CBD), see our CBD bioavailability guide
Side Effects and Drug Interactions
Both CBG and CBD have relatively mild side effect profiles, but there are differences worth knowing.
CBD
- Drowsiness at higher doses
- Diarrhea and fatigue in a subset of users, especially at 200+ mg/day
- Decreased appetite
- Drug interactions: CBD inhibits cytochrome P450 enzymes CYP3A4 and CYP2C9, which metabolize many prescription medications. If you take blood thinners, anti-seizure drugs, immunosuppressants, or certain antidepressants or heart medications, ask your doctor or pharmacist before starting CBD. This is the most consequential practical concern
- WHO 2018 concluded pure CBD has good safety and no abuse potential
CBG
- Cuttler 2024 reported no significant adverse events at 20mg compared to placebo
- Possible mild dry mouth (consistent with other cannabinoids)
- Possible drowsiness at higher doses (inconsistent with Cuttler findings but reported anecdotally)
- Drug interactions: Less characterized than CBD. CBG is expected to have similar CYP450 inhibition potential. Same precaution applies: ask a doctor if you’re on prescription medications
For the drug test specifics on both compounds, read our guide on whether CBD shows up on a drug test.
Cost and Availability
CBD is the cheapest, most widely available cannabinoid in the consumer market. Mass-market CBD isolate can be produced for cents per milligram at scale. Commercial CBD tinctures, gummies, and capsules are sold across most US states at competitive prices.
CBG typically costs 2 to 5 times more per milligram than CBD. The production reality: CBG is present in very low amounts in mature cannabis flower, so specialty cultivation (CBG-dominant strains harvested early) or chromatographic isolation from concentrated extracts is required. Both paths increase cost.
The commercial catch: because CBG is expensive, many products labeled “CBG” contain very low amounts (5mg or less per serving) to keep cost down while allowing the CBG branding. A 20mg CBG product priced competitively with CBD would lose money for most brands. Matching the Cuttler 2024 research dose requires either buying higher-dose CBG products (15-25mg per serving, typically priced at a premium) or taking multiple servings of lower-dose products, which gets expensive.
Legal Status and Drug Tests
Both CBG and CBD are legal at the federal level in the United States under the 2018 Farm Bill, as long as the source plant contains less than 0.3% delta-9 THC by dry weight. Both are sold openly in most states. State-level regulations vary for cannabinoid food additives and intoxicating hemp products, but non-intoxicating CBG and CBD are broadly legal.
A major federal change is coming on November 12, 2026, when H.R. 5371 Section 781 takes effect and redefines federal hemp. The change primarily targets intoxicating hemp products (delta-8 THC, high-THCA flower, and similar), and non-intoxicating CBG and CBD products are expected to remain broadly legal. For the full federal context, see our Delta-8 legal states guide.
For drug testing, neither CBG nor CBD is the target of standard THC drug tests. Pure isolates (CBG isolate or CBD isolate) with certificates of analysis showing 0 detectable THC should not trigger a positive result. Full-spectrum and broad-spectrum products for either cannabinoid contain trace THC (up to 0.3% by dry weight) that can produce a positive test with regular use.
Which Should You Use? A Decision Framework
Cut through the marketing. Here’s a research-informed framework.
Choose CBD if:
- You want the cannabinoid with the deepest evidence base
- You value FDA approval signals (only CBD has Epidiolex)
- Cost matters (CBD is typically cheaper per mg)
- You’re treating epilepsy under medical supervision
- You want general wellness support rather than a specific focus or anxiety target
- You need sustained daily use and want a compound with long-duration data
- You’re okay with a compound that doesn’t produce “focus” or pro-cognitive effects at standard doses
Choose CBG if:
- Your specific goal is acute anxiety reduction at low doses
- You’re interested in the “clear-headed calm” or “focus” subjective profile
- You want to prioritize the cannabinoid with the best-designed recent single trial (Cuttler 2024)
- You’re okay paying more for a less-tested compound
- You want verbal memory support (unique to CBG in current data)
- You’re experimenting with minor cannabinoids and want the one with the strongest recent signal
Consider both (sequentially or combined) if:
- You’ve tried one alone and want to layer
- Your goal spans anxiety (both) + focus (CBG) + chronic inflammation (CBD)
- You’re comfortable with a cost premium for combination products
- You’re willing to experiment given the limited head-to-head data
A pragmatic starting path: if you’ve never used either, start with CBD because the evidence is deeper and the cost is lower. If CBD works for you, stay there. If it doesn’t address your specific concern (particularly focus or acute anxiety without sedation), try CBG as the targeted second choice. Combining them is a reasonable third step if single compounds haven’t delivered.
Frequently Asked Questions
CBG (cannabigerol) is the biosynthetic precursor that the cannabis plant converts into CBD (cannabidiol) and other cannabinoids. CBD binds the CB1 cannabinoid receptor as a negative allosteric modulator and engages 5-HT1A, TRPV1, and FAAH pathways. CBG is a weak partial agonist at CB1 and CB2 and distinctively engages α-2 adrenergic receptors. CBD has FDA approval (Epidiolex) and a much deeper evidence base; CBG has one human clinical trial (Cuttler 2024) showing acute anxiety reduction and memory enhancement at 20mg.
“Stronger” isn’t a useful framing because the two cannabinoids work through different receptor systems and have different use cases. For acute anxiety reduction, the Cuttler 2024 CBG trial produced a measurable effect at 20mg, which is a lower effective dose than comparable CBD trials typically use. For general-purpose daily cannabinoid support, CBD has more evidence. For verbal memory and focus specifically, CBG has better evidence. Neither is categorically stronger than the other; they’re just different.
No. CBG binds the CB1 cannabinoid receptor (responsible for THC’s psychoactive effects) only weakly, and it does not produce intoxication at typical doses. The Cuttler 2024 trial specifically measured subjective drug effects at 20mg and found no evidence of impairment compared to placebo. Like CBD, CBG is categorized as non-psychoactive for all practical purposes.
Yes. They engage different but overlapping receptor systems, so combining them is mechanistically reasonable and safety data suggests acceptable tolerability. A 2023 pilot study tested a CBD + CBG beverage powder for muscle soreness recovery without notable adverse events. However, no RCT has demonstrated that the combination outperforms either compound alone on specific outcomes. The Cuttler 2024 CBG trial did not test CBG+CBD combinations.
CBG is present in very low amounts in mature cannabis flower (typically under 1% of total cannabinoids), because the plant converts most CBGA into THCA, CBDA, and CBCA as it matures. To produce commercial CBG, manufacturers either grow specialty CBG-dominant strains harvested early before conversion happens, isolate CBG chromatographically from concentrated extracts, or use biosynthesis. All of these paths are more expensive than extracting CBD from hemp flower that’s dominant in CBD.
Both have human evidence. For acute anxiety at a low dose, the Cuttler 2024 CBG trial (N=34, 20mg, 26.5% reduction at 20-60 min) is the highest-quality recent data. For broader daily anxiety management, CBD has more total research including the Shannon 2019 case series (N=72, 79.2% improved in month 1) plus several smaller randomized trials. If you want the best-designed single acute trial at a practical dose, CBG has a claim. If you want depth of evidence, CBD has a claim. Both are defensible choices; sequential trials are a reasonable strategy.
Picking Your Cannabinoid
CBG vs CBD isn’t really a contest. They’re different compounds with different evidence bases and different use cases. The smart move is matching the compound to your goal: CBD for general wellness, chronic use, broad-evidence support, or epilepsy under medical care. CBG for acute anxiety at low doses, focus support, or verbal memory assist. Both for combination experiments when single compounds haven’t delivered.
Whichever direction you go, buy from brands that publish full third-party certificates of analysis so you know the actual cannabinoid content per serving matches the label. TribeTokes publishes COAs on every batch. Our CBD vape cartridges give you predictable dosing, and for the underlying science, our companion articles on CBG benefits and CBD vs THC cover each cannabinoid in more depth.
For the related comparison of CBN vs CBD for sleep, see our CBN vs CBD sleep guide. For the CBD format decision (full spectrum vs broad spectrum vs isolate), our spectrum comparison is the companion reference. For delivery method bioavailability, see the bioavailability guide. And for terpene effects that often layer on top of cannabinoid products, our terpenes guide breaks down the common ones.
Lab tested. Transparent. No cannabinoid claims without a citation.
Shop TribeTokes Lab-Tested Hemp Products
Full third-party COAs on every batch. Woman-owned since 2017. Research-aligned cannabinoid dosing.