

CBD and THC are the two most studied cannabinoids in hemp and cannabis. They share the same molecular formula. They come from the same plant. And they produce almost completely opposite effects in your body. One gets you high. The other doesn’t. One is federally legal in most forms. The other is mostly not. One has one FDA-approved medication; the other has three. This guide walks through what’s actually the same, what’s actually different, what the research says about each, and how to decide which one fits whatever you’re trying to do.
🧪 Lab Tested | 👩💼 Woman-Owned | 🏆 Est. 2017
IN THIS GUIDE
- The Short Answer
- What Is CBD?
- What Is THC?
- The Chemistry: Same Formula, Different Molecule
- How They Interact with Your Endocannabinoid System
- What the Research Says About Benefits
- Side Effects Compared
- Legal Status
- Drug Test Implications
- Dosing Differences
- Can You Use Them Together?
- Which to Use When: A Decision Framework
- Frequently Asked Questions
- Shop TribeTokes
CBD vs THC at a Glance
| Psychoactive? | CBD: no. THC: yes |
| Molecular formula | Both are C21H30O2. Same atoms, different arrangement |
| CB1 receptor action | CBD: negative allosteric modulator. THC: partial agonist (Ki 10 nM) |
| Federal legal status | CBD: legal if hemp-derived under 2018 Farm Bill. THC: Schedule I (with narrow hemp exception for <0.3%) |
| Drug test risk | CBD isolate: minimal. Full-spectrum CBD: possible. THC: yes, always |
| FDA-approved drug forms | CBD: Epidiolex (2018). THC: Marinol, Syndros, Cesamet (since 1985) |
| Addiction potential | CBD: per WHO 2018, no abuse potential in pure form. THC: yes, especially with heavy/adolescent use |
| Typical use cases | CBD: daytime, calm, sleep support. THC: evening, pain, appetite, recreational |
| Combined use | May enhance each other’s effects while softening THC’s side effects (entourage effect) |
The Short Answer
CBD (cannabidiol) and THC (tetrahydrocannabinol) are both naturally occurring compounds in the cannabis plant, and they’re the two most common cannabinoids in commercial products. They’re chemically almost identical: both have the molecular formula C21H30O2, meaning they contain exactly the same atoms arranged in slightly different ways. That small structural difference changes everything about how they interact with your body.
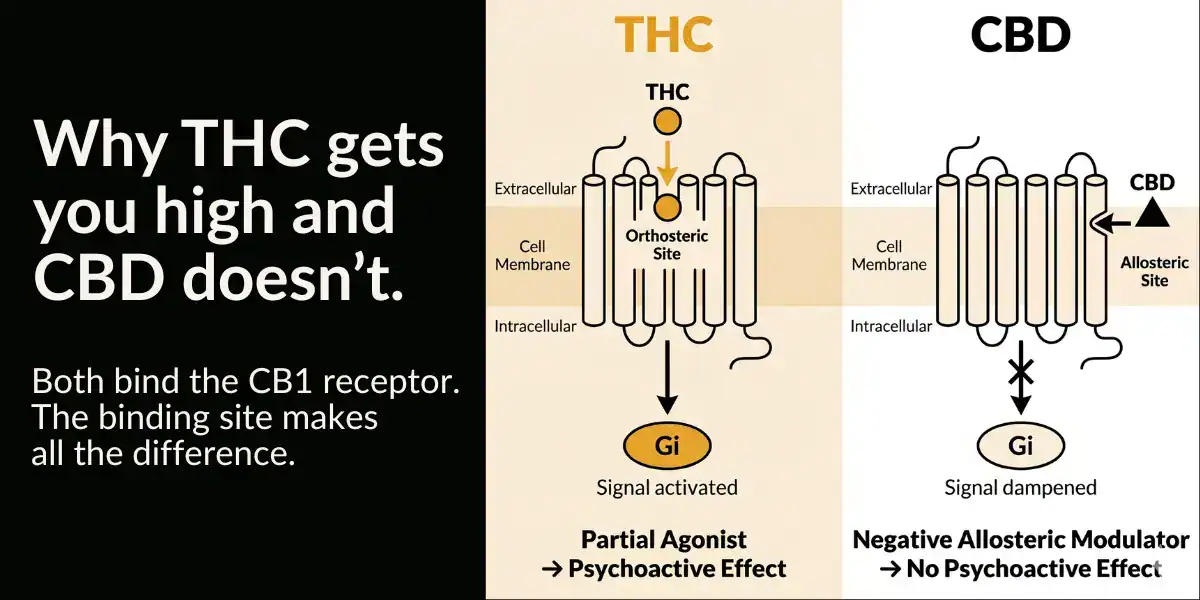
THC binds directly to CB1 cannabinoid receptors in your brain and produces the psychoactive effects people associate with cannabis: euphoria, altered perception, appetite stimulation, and the classic high. CBD does not bind to CB1 the same way and doesn’t produce those effects. Instead, CBD modulates the receptor from a different site (technically, it’s a negative allosteric modulator) and interacts with several other receptor systems in ways that have been studied for anxiety, seizures, inflammation, and sleep.
If you want to get high, you want THC. If you want the cannabinoid experience without intoxication, you want CBD. If you want a drug-test-safe option, you want CBD isolate specifically. If you want to combine them, that’s also an option and there’s research suggesting the combination may work better than either one alone. The rest of this guide goes deep on why.
What Is CBD?
CBD is short for cannabidiol. It’s one of over 100 cannabinoids produced by the Cannabis sativa plant. In hemp, CBD is the dominant cannabinoid, and hemp is legally defined as cannabis with less than 0.3% delta-9 THC by dry weight. That definition is why hemp-derived CBD products are federally legal under the 2018 Farm Bill.
CBD doesn’t get you high. It has no significant psychoactive effect at normal doses. At very high doses it can produce mild drowsiness or relaxation, but nothing like the intoxication from THC. Some people describe a subtle calming effect; others feel nothing at all, which is part of what makes CBD a confusing product category to navigate.
CBD is widely available as oils and tinctures, capsules, gummies, topicals, vape cartridges, and beverages. Within each form, you’ll see “full spectrum,” “broad spectrum,” or “isolate” designations, which refer to what else is in the product besides CBD. Our guide on full spectrum vs broad spectrum vs isolate covers the decision between those three formats.
CBD has one FDA-approved prescription form: Epidiolex, a purified plant-derived cannabidiol oral solution. Epidiolex was approved by the FDA on June 25, 2018 for the treatment of seizures associated with Dravet syndrome and Lennox-Gastaut syndrome in patients 2 years and older, and its approval was later expanded to include tuberous sclerosis complex. It’s the first (and as of this writing, only) FDA-approved drug derived from the cannabis plant.
What Is THC?
THC is short for delta-9 tetrahydrocannabinol, the primary psychoactive compound in cannabis. THC is what produces the high, the altered perception, the appetite stimulation, and the characteristic euphoria of cannabis consumption. It’s the compound that has driven cannabis use for thousands of years and the compound that makes cannabis classified as a Schedule I controlled substance at the federal level in the United States.
THC’s effects come from its interaction with the CB1 cannabinoid receptors in the brain, where it acts as a partial agonist with a binding affinity of approximately Ki = 10 nM. The effects are dose-dependent: a small amount produces mild euphoria and relaxation, a moderate amount produces the classic high with time distortion and heightened sensory perception, and a large amount can produce anxiety, paranoia, and disorientation.
THC also comes in several structurally related forms. Delta-9 THC is the naturally dominant form in mature cannabis. Delta-8 and delta-10 THC are minor cannabinoids that occur naturally in small amounts, but most commercial delta-8 is produced by chemically converting CBD (and is subject to a federal ban effective November 12, 2026 under H.R. 5371). THCa (tetrahydrocannabinolic acid) is the non-psychoactive precursor that converts to THC when heated. For the compound-specific comparison, our THCa vs THC guide breaks it down.
Unlike CBD, THC has multiple FDA-approved prescription forms. According to the FDA’s cannabis research and drug approval overview, three synthetic cannabis-related drug products have been approved: Marinol and Syndros (both dronabinol) and Cesamet (nabilone). Dronabinol is synthetic THC that’s been FDA-approved since 1985 for two indications: chemotherapy-induced nausea and vomiting in patients who don’t respond to conventional antiemetics, and anorexia associated with weight loss in patients with HIV/AIDS. Nabilone (Cesamet) is a synthetic THC analog approved for the same chemotherapy nausea indication. None of these are smoked or vaped; they’re oral medications taken as prescribed.
The Chemistry: Same Formula, Different Molecule
Here’s the part that surprises people. CBD and THC have the same molecular formula: C21H30O2. They contain exactly the same number of carbon atoms (21), hydrogen atoms (30), and oxygen atoms (2). They’re structural isomers, which means they’re made of the same atoms but arranged in different ways.
The key difference is one ring closure. THC has a closed ring structure on one end of the molecule, which creates a three-dimensional shape that fits neatly into the CB1 receptor’s active site. CBD has an open ring in the same location, which prevents it from fitting into CB1 the same way. That single structural feature is why one gets you high and the other doesn’t.
The pharmacological consequences flow from the structure. THC binds to CB1 receptors like a key in a lock, activating downstream signaling that produces intoxication, altered perception, and the euphoric high. CBD doesn’t fit the lock. It binds to a different part of the receptor and, through allosteric modulation, actually changes how the receptor responds to other ligands (including THC itself).
Both molecules are lipophilic (fat-soluble), which is why cannabinoids are typically formulated in oils, taken with fatty meals for better absorption, and stored in body fat for extended periods after use.
How They Interact with Your Endocannabinoid System
Your body has a biological signaling network called the endocannabinoid system, which includes two primary receptors (CB1 and CB2), endogenous cannabinoids your body makes (anandamide and 2-AG), and the enzymes that build and break down those compounds. Both CBD and THC interact with this system, but in different ways.
THC at the CB1 receptor
THC is a partial agonist at the CB1 receptor, which is densely expressed in the central nervous system (particularly in areas involved in memory, mood, perception, pain, and motor control). When THC binds to CB1, it partially activates the receptor. “Partial” matters here: full agonists (like synthetic cannabinoids, sometimes called K2 or Spice) activate the receptor more strongly and are associated with much more severe adverse effects. THC’s partial agonism is one reason it’s substantially safer than synthetic analogs, though not without risks.
THC also binds to CB2 receptors (which are primarily in immune tissue and the gut) with similar but slightly weaker affinity (Ki = 24 nM at CB2). CB2 activation is associated with anti-inflammatory effects and doesn’t produce the classic “high.”
CBD at the CB1 receptor
CBD doesn’t bind to the main CB1 active site the way THC does. Instead, a 2015 study by Laprairie and colleagues in the British Journal of Pharmacology found that CBD acts as a negative allosteric modulator of CB1. In plain English: CBD binds to a different site on the receptor and reduces how strongly other ligands (including THC) activate it. That’s one proposed mechanism for why combining CBD with THC can soften THC’s side effects while preserving some of its therapeutic benefit.
CBD everywhere else
CBD is a busy molecule beyond CB1. It interacts with:
- Serotonin 5-HT1A receptors, which may contribute to its effects on anxiety and mood
- TRPV1 receptors (vanilloid receptors, same ones activated by capsaicin), which are involved in pain and body temperature
- GPR55 (sometimes called the “third cannabinoid receptor”), with complex and still-being-mapped effects
- FAAH enzyme inhibition, which slows the breakdown of your body’s own endocannabinoid anandamide
- PPAR-gamma receptors, involved in metabolism and inflammation
This multi-receptor profile is part of why CBD has been studied for such a wide range of conditions. It’s also why the clinical effects of CBD aren’t well predicted by simple dose-response curves at a single receptor.
What the Research Says About Benefits
Any conversation about cannabinoid benefits has to distinguish between what’s FDA-approved (high evidence bar) and what’s been studied in smaller trials or is commonly reported by users (much wider range of reliability).
CBD benefits with strong evidence
- Treatment-resistant epilepsy in specific syndromes. Epidiolex has FDA approval based on placebo-controlled trials showing significant seizure reduction in Dravet syndrome, Lennox-Gastaut syndrome, and tuberous sclerosis complex
- General safety profile. The WHO Expert Committee on Drug Dependence concluded in 2018 that pure CBD does not appear to have abuse potential or cause harm, is generally well tolerated, and does not produce physical dependence
CBD uses with mixed or preliminary evidence
- Anxiety: Small human trials (mostly short-term) have shown CBD may reduce situational anxiety at specific doses. Longer-term data is limited
- Sleep: Some studies suggest CBD may improve sleep in people with certain conditions; results are inconsistent across studies
- Chronic pain: Animal models show anti-inflammatory and analgesic effects; human clinical data is mixed
- Inflammation: Clear preclinical evidence; clinical translation is uneven
THC benefits with strong evidence
- Chemotherapy-induced nausea and vomiting. Dronabinol and nabilone are FDA-approved for this indication in patients who have failed conventional antiemetic treatment
- Anorexia and weight loss in HIV/AIDS. Dronabinol has FDA approval for this specific indication
THC uses with mixed or preliminary evidence
- Chronic pain: Several meta-analyses show moderate effects for neuropathic pain in particular; results vary by pain type
- Multiple sclerosis spasticity: Sativex (a THC+CBD oromucosal spray) is approved in multiple countries (not the US) for MS spasticity
- Sleep: Short-term benefit reported; tolerance develops with regular use
- Glaucoma: THC reduces intraocular pressure but only for 3 to 4 hours, making it impractical as primary treatment
None of this is a recommendation to use cannabinoids to treat a medical condition. If you’re considering CBD or THC for a specific health issue, talk to a doctor. The FDA-approved drug forms (Epidiolex, Marinol, Syndros, Cesamet) require prescriptions for a reason. Over-the-counter hemp products are not substitutes for medical treatment.
Side Effects Compared
Neither compound is free of side effects, and the side-effect profiles are very different.
THC side effects
- Short-term impaired memory and cognition
- Impaired motor coordination and reaction time (do not drive)
- Dry mouth (“cottonmouth”) and red eyes
- Increased heart rate
- Anxiety, paranoia, or panic at high doses
- Risk of cannabis use disorder (approximately 9% of lifetime users, higher for those who start in adolescence)
- Potential for acute psychotic symptoms in people predisposed to psychosis
- Cannabinoid hyperemesis syndrome in rare chronic heavy users
CBD side effects
The WHO 2018 review reported that in clinical trials, adverse events affecting more than 10% of patients were somnolence (drowsiness), decreased appetite, diarrhea, fatigue, and convulsion. The convulsion note is specific to patients with severe pediatric epilepsy being treated with high-dose CBD; it’s not something most adult users of over-the-counter CBD would experience.
The bigger CBD concern is drug-drug interactions. CBD inhibits cytochrome P450 enzymes (particularly CYP3A4 and CYP2C9), which are the same enzymes that metabolize a long list of common prescription medications. If you take blood thinners, anti-seizure drugs, immunosuppressants, or certain heart medications, CBD can affect their blood levels. If you’re on prescription medication, ask your doctor or pharmacist before starting CBD.
Legal Status
Federal and state laws diverge, and the rules changed significantly in late 2025.
CBD legal status
Hemp-derived CBD is federally legal under the 2018 Farm Bill as long as the source plant is defined as hemp (less than 0.3% delta-9 THC by dry weight). The FDA regulates CBD as a drug (Epidiolex) and considers other CBD products to be unapproved drugs, supplements, or food additives depending on marketing and form. States vary on how they regulate CBD in food, beverages, and cosmetics, but possession and sale of hemp-derived CBD is broadly legal across most of the country.
THC legal status
Delta-9 THC above 0.3% by dry weight is a Schedule I controlled substance at the federal level. State laws vary: some states have legalized recreational adult-use cannabis, some have medical cannabis programs only, and some prohibit cannabis entirely. Hemp-derived delta-9 products (typically beverages or gummies that stay under 0.3% by dry weight) occupied a gray zone until the November 2025 federal hemp redefinition, which is set to take effect on November 12, 2026.
The November 12, 2026 federal change
H.R. 5371, signed into law November 12, 2025, rewrites the federal definition of hemp. Starting November 12, 2026, the threshold shifts from a delta-9-only standard to a total-THC standard, adds a 0.4mg per-container cap on total THC in finished products, and excludes chemically converted cannabinoids like Delta-8. For the full impact and state-by-state picture, our Delta-8 legal states guide covers the details.
Drug Test Implications
This is the practical question that affects employment, probation, and legal situations.
THC will absolutely show up on a drug test. Standard workplace and pre-employment drug tests measure THC-COOH, the main inactive metabolite of delta-9 THC. Any form of THC consumption (flower, vape, edible, tincture, topical) that produces any meaningful blood level will also produce detectable THC-COOH. Detection windows range from about 3 days for a single use to 30+ days for daily heavy use.
Pure CBD (isolate) should not trigger a positive drug test. The CBD molecule itself isn’t what the test looks for, and a verified isolate product with 0 detectable THC on its certificate of analysis doesn’t produce THC-COOH. In theory, isolate is the only drug-test-safe CBD option.
Full-spectrum CBD can trigger a positive test. The trace delta-9 THC allowed in full-spectrum products (up to 0.3% by dry weight) can accumulate with regular use and produce measurable THC-COOH levels. Broad-spectrum CBD carries lower risk than full-spectrum but isn’t zero-risk because “broad spectrum” labeling has varying standards.
For the complete detection-test breakdown, read whether CBD shows up on a drug test. For the THC side of the equation, our Delta-8 drug test guide covers the science of how intoxicating hemp cannabinoids get detected (the principles apply equally to regular delta-9).
Dosing Differences
Typical therapeutic doses of CBD and THC are dramatically different.
THC dosing
THC is potent in milligram quantities. A starting dose for a first-time edible user is typically 2.5 to 5 milligrams. An experienced user might take 10 to 25mg per serving. For smoked or vaped cannabis, dose-per-inhalation is harder to measure precisely but produces effects in the same low-milligram range.
CBD dosing
CBD is effective at much higher doses in clinical research. Epidiolex treatment for epilepsy starts at 2.5 mg/kg twice daily and titrates up to 10 mg/kg twice daily, which for an adult means doses in the range of 200 to 1,000+ mg per day. Over-the-counter CBD doses are typically far lower (10 to 50 mg per serving), which is why results from consumer products are inconsistent compared to the clinical evidence at higher doses.
The practical takeaway: if you’re comparing a 25mg THC gummy to a 25mg CBD gummy, you’re not comparing equivalent doses of equivalent drugs. You’re comparing a noticeable dose of THC to a below-therapeutic-dose of CBD.
Can You Use Them Together?
Yes, and there’s research suggesting the combination may work differently than either alone. This is the area where the “entourage effect” hypothesis gets most interesting.
A 2011 review by Ethan Russo in the British Journal of Pharmacology argued that CBD softens some of THC’s adverse effects (anxiety, paranoia, memory impairment) while preserving some of its therapeutic benefit. Sativex, a combination CBD+THC oromucosal spray approved in many countries (not the US), is based on this principle: the 1:1 CBD:THC ratio was designed to produce therapeutic effects for MS spasticity and cancer pain with fewer psychoactive side effects than THC alone.
CBD’s role here appears to be partly allosteric modulation at CB1 (reducing THC’s binding efficacy) and partly independent effects via its other receptor targets. The combination is pharmacologically real, not just marketing.
For consumer products, this translates into a practical question: if you want a less intense THC experience, pairing with CBD can help. Common ratios in commercial products are 1:1 (balanced), 2:1 or 3:1 CBD to THC (CBD-dominant, milder effects), or 1:2+ THC to CBD (THC-dominant, strong high with some CBD softening). Our guide on the entourage effect covers the receptor-level mechanisms in more detail.
Which to Use When: A Decision Framework
Cut through the marketing. Here’s a practical framework based on what these compounds actually do differently.
Consider CBD if:
- You want cannabinoid effects without getting high
- You can’t afford a positive drug test (and specifically isolate)
- You’re looking for daytime support that won’t impair function
- You’re in a state where THC is illegal or restricted
- You’re interested in the FDA-approved epilepsy indications and working with a doctor
- You want to try cannabinoids for anxiety or sleep at a low barrier to entry
Consider THC if:
- You want the classic cannabis experience (recreational or experiential)
- You’re in a state where cannabis is legal
- You’re being treated for chemotherapy nausea or HIV/AIDS-associated anorexia and your doctor prescribes dronabinol or nabilone
- You have chronic pain that hasn’t responded to other approaches and you’re working with a provider
- You’re okay with the drug-test risk and the impairment window
- You’re not in a safety-sensitive role or a zero-tolerance workplace
Consider combining them if:
- You want THC’s effects but want to soften the psychoactive intensity
- You’ve had past anxiety reactions to THC and want to try it again with a CBD buffer
- You’re looking at a balanced cannabis or hemp product for sleep or pain
- You live in a state with a legal market and want to experiment with different CBD:THC ratios
A practical rule: Start with CBD if you’ve never used cannabinoids. If CBD alone doesn’t deliver what you’re looking for after a fair trial, consider a balanced CBD:THC product. Save high-THC products for specific situations where you know what you’re getting into.
Frequently Asked Questions
No. CBD is non-intoxicating. Some people notice mild relaxation or drowsiness at higher doses, but CBD does not produce the euphoria, altered perception, or impaired cognition associated with THC. At the CB1 receptor, CBD acts as a negative allosteric modulator rather than a direct activator, which is why it doesn’t produce a high.
Pure CBD isolate with a certificate of analysis showing 0 detectable THC should not trigger a positive drug test. Full-spectrum CBD (which contains trace delta-9 THC up to 0.3% by dry weight) can trigger a positive, especially with regular use. Broad-spectrum CBD carries lower but not zero risk. If drug testing matters in your situation, use verified CBD isolate or skip CBD entirely.
THC above 0.3% delta-9 by dry weight is federally Schedule I. At the state level, adult-use cannabis is legal in many states, medical cannabis in many more, and prohibited in several. Hemp-derived THC products (beverages, edibles compliant with the 0.3% threshold) occupy a gray zone that changes federally on November 12, 2026 under H.R. 5371 Section 781. Check your state before purchasing.
The honest answer is “it depends on the person and the dose.” Low-dose CBD has been studied for situational anxiety and has shown some benefit in short-term trials. THC is biphasic for anxiety: low doses may reduce anxiety, higher doses can worsen it significantly. THC alone is not a first-choice intervention for anxiety because of that dose-response pattern. CBD’s main benefit is a wider therapeutic window and minimal intoxication. Talk to a clinician for specific guidance.
Yes. Research suggests CBD can reduce some of THC’s side effects (anxiety, paranoia, memory issues) while preserving some therapeutic benefit. Balanced 1:1 CBD:THC products exist in state-legal cannabis markets for this reason. Sativex, a combination CBD+THC product approved in multiple countries (not the US), is based on this principle. Consumer products often come in 2:1, 1:1, or 1:2 ratios depending on desired effect.
THC has more clinically significant short-term side effects: impaired cognition and motor skills, anxiety and paranoia at high doses, increased heart rate, and a ~9% lifetime risk of cannabis use disorder. CBD’s main practical concerns are drug-drug interactions (especially with medications metabolized by CYP3A4 or CYP2C9), occasional drowsiness, and diarrhea at higher doses. The WHO concluded in 2018 that pure CBD has no abuse potential. If you’re on prescription medications, CBD carries interaction risk that THC does not carry in the same way.
TribeTokes and the CBD/THC Question
The right choice between CBD and THC isn’t about which is “better.” It’s about what you need the product to do and what trade-offs you can accept. If you need drug-test safety, CBD isolate is the path. If you need to stay sharp during the day, CBD works. If you want the classic cannabis experience and your situation allows it, THC is the compound. If you want some of both effects, combining them is a real, research-supported option.
Whatever you pick, buy from brands that publish full third-party certificates of analysis. TribeTokes tests every batch and publishes the full cannabinoid and terpene breakdown. Our CBD vape cartridges give you predictable dosing with lab-verified content, and our THCa vape collection covers the THC side for adults in states where it’s legal.
Want to go deeper on specific topics? Our full spectrum vs broad spectrum vs isolate guide helps you pick the right CBD format. The THCa vs THC guide covers the THC-side chemistry. And our terpenes guide walks through the aromatic compounds that shape how each cannabinoid actually feels.
Lab tested. Transparent. No claims we can’t back up.
Shop TribeTokes Lab-Tested CBD and THCa
Full third-party COAs on every batch. Woman-owned since 2017. Transparent cannabinoid and terpene reporting on every product.