

You ate a 10mg gummy 45 minutes ago. You feel nothing. You are very close to eating another one. Before you do, read this. When you swallow a THC edible, it takes anywhere from 30 to 120 minutes to hit because it has to travel through your stomach, your small intestine, and your liver before a single molecule reaches your brain. Each stage changes how strong the high feels and how long it lasts. This guide walks through every stop on that journey so you know what your body is actually doing, and why 5mg of smoked THC feels nothing like 5mg in a cookie.
🧪 Lab Tested | 👩💼 Woman-Owned | 🏆 Est. 2017
IN THIS GUIDE
- The Journey: From Bite to Brain
- Stage 1: Your Mouth and Stomach
- Stage 2: The Small Intestine (Where Absorption Happens)
- Stage 3: The Portal Vein and Your Liver
- Stage 4: 11-Hydroxy-THC Enters Your Bloodstream
- Why Oral Bioavailability Is So Low
- How Food Changes Everything
- CYP2C9 Variability: Same Dose, Different People
- What THC Does to Your Gut Beyond Getting You High
- The Enterohepatic Recirculation Loop
- How Long THC Stays in Your Body After Digestion
- How to Time Edibles for the Best Experience
- Frequently Asked Questions
- Shop TribeTokes
THC Digestion at a Glance
| Typical onset (edibles) | 30 to 120 minutes after swallowing |
| Peak plasma THC | 1 to 3 hours post-ingestion |
| Total duration | 4 to 8 hours, up to 12 at high doses |
| Oral bioavailability | 4 to 12 percent (McGilveray 2005) |
| Inhaled bioavailability (for contrast) | Around 30 percent |
| Key liver enzymes | CYP2C9 and CYP3A4 convert Δ9-THC into 11-hydroxy-THC |
| Food effect (Lunn 2019) | A meal delays Tmax about 3.5-fold and raises AUC 2.7-fold at 5mg |
| Safety rule | Start low, go slow. Wait a full 2 hours before considering another dose |
The Journey: From Bite to Brain
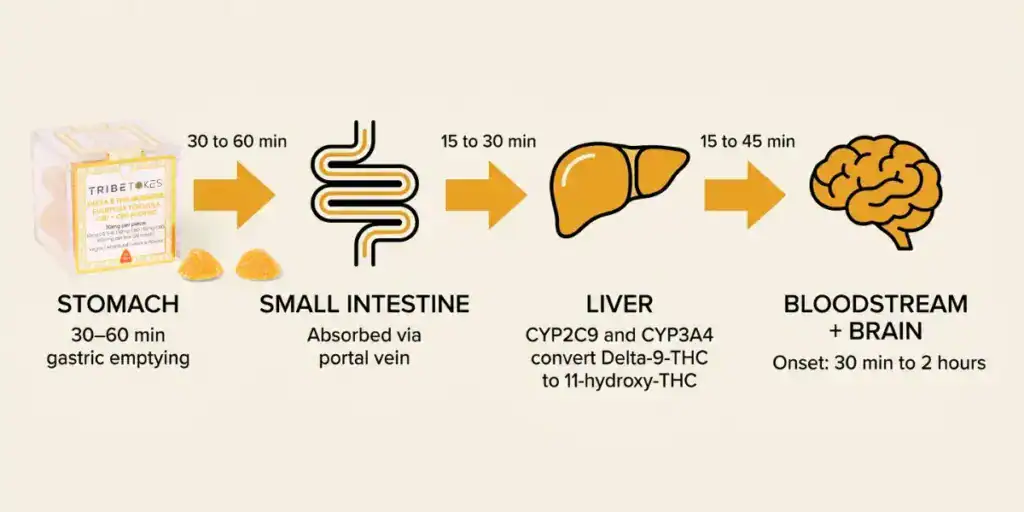
When you smoke or vape cannabis, THC jumps from your lungs into your bloodstream in about 10 seconds. Digestion is a slower, weirder story. An edible passes through four distinct stages before you feel anything, and at each stage, the chemistry changes. Here is the full path.
| Stage | Location | What Happens | Time |
| 1 | Mouth and stomach | Edible breaks down. Almost no THC absorbs yet. Gastric emptying pushes it onward. | 0 to 60 min |
| 2 | Small intestine | Most THC absorbs through the intestinal wall into the portal venous blood and lymph. | 30 to 120 min |
| 3 | Liver (first-pass) | CYP2C9 and CYP3A4 convert a large share of Δ9-THC into 11-hydroxy-THC. | Ongoing during absorption |
| 4 | Systemic circulation | Surviving Δ9-THC plus 11-hydroxy-THC reach the brain. You feel the high. | Peak at 1 to 3 hr |
Now let’s walk through what happens at each stage, and why the details matter for how your edible actually feels.
Stage 1: Your Mouth and Stomach
The journey starts the moment you chew. A small amount of THC from certain products (especially infused candies or tinctures held under the tongue) can absorb through the mucous membranes of your mouth. For a gummy you chew and swallow in 10 seconds, that buccal absorption is negligible. Almost everything goes down the pipe.
Your stomach is not where THC gets absorbed in any meaningful way. Stomach pH sits around 1.5 to 3.5, which is great for breaking down proteins and killing pathogens and not great for absorbing fat-soluble cannabinoids. What your stomach does instead is mechanical: it churns, mixes, and breaks the edible down into a soupy liquid called chyme. Along the way, it separates the THC from the fats and sugars it was formulated with.
The big variable at this stage is gastric emptying time: how fast your stomach pushes chyme into the small intestine. On an empty stomach, that happens in roughly 20 to 60 minutes. After a full meal, it can take 2 to 4 hours. This is the single biggest reason two people can eat identical 10mg gummies and one feels it at 45 minutes while the other waits 2 hours.
If you’ve ever wondered why the same edible sometimes hits in 30 minutes and sometimes in 90, this is where most of that variance comes from. Nothing has absorbed yet. Your stomach is just waiting for its turn to pass the chyme along.
Stage 2: The Small Intestine (Where Absorption Happens)
The small intestine is the main event. This is where the majority of oral THC crosses from your gut into your blood. Your small intestine has a surface area of roughly 30 square meters once you account for the folds, villi, and microvilli that line its walls. That is the biological equivalent of a large studio apartment designed entirely to absorb nutrients and fat-soluble molecules. THC qualifies.
Because THC is lipophilic (fat-loving, water-hating), it hitches a ride with dietary fats. Your liver makes bile, your gallbladder stores it, and when fats enter the small intestine, bile gets released to emulsify them into tiny droplets called micelles. THC dissolves into those micelles along with the fats it was packaged with, and the micelles deliver their cargo to the intestinal wall for absorption.
Once absorbed, THC can take two routes out of the gut: most of it enters the portal venous blood, which drains directly to the liver. A smaller portion enters the lymphatic system via chylomicrons (fat-carrying particles), which eventually dumps into general circulation, bypassing the liver on the first pass.
This dual-path absorption is part of why edibles have such variable timing. The lymphatic fraction avoids immediate liver metabolism, which can contribute to a faster front end of the high for some people. The portal vein fraction is the much bigger share and heads straight for the liver.
Stage 3: The Portal Vein and Your Liver (First-Pass Metabolism)
Here is where oral THC becomes a completely different drug than inhaled THC. Before any edible-derived THC reaches the rest of your body, it passes through your liver. This is called first-pass metabolism, and it is the most important concept in understanding why edibles work the way they do.
Your liver contains a family of enzymes called cytochrome P450 (CYP450) that break down most drugs, toxins, and foreign compounds. For THC, two specific CYP enzymes do most of the work: CYP2C9 and CYP3A4. According to the published pharmacology on THC metabolism, these enzymes convert Δ9-THC into its primary active metabolite, 11-hydroxy-THC (11-OH-THC), which is then further oxidized into the inactive 11-nor-9-carboxy-THC (THC-COOH, the compound drug tests look for).
Two things happen during first-pass that matter for how you feel:
- A big chunk of Δ9-THC is destroyed before it reaches your blood. This is why oral bioavailability is so much lower than inhaled. When you smoke, THC goes lungs to blood to brain with no liver gatekeeping.
- A large share of Δ9-THC converts into 11-hydroxy-THC. When you inhale, your blood carries mostly Δ9-THC with small amounts of 11-OH-THC formed later. With edibles, the liver pumps out 11-hydroxy-THC up front, often at levels comparable to or exceeding the parent Δ9-THC concentration.
So oral THC doesn’t just give you “less” THC in your blood. It gives you a different mix of molecules than what inhalation produces. That mix is what makes edibles feel distinct.
Stage 4: 11-Hydroxy-THC Enters Your Bloodstream
After the liver does its job, a cocktail of surviving Δ9-THC plus freshly made 11-hydroxy-THC spills out into your general circulation. Both molecules cross the blood-brain barrier, but 11-OH-THC has some interesting properties that explain the “edible feel.”
At the CB1 receptor (the main cannabinoid receptor in your brain), 11-hydroxy-THC binds with much higher affinity than Δ9-THC. The published binding data puts 11-OH-THC’s Ki at roughly 0.37 nM, compared to about 35 nM for Δ9-THC. In plain English, the 11-hydroxy form grabs onto the receptor about 95 times more tightly.
That said, binding affinity is not the whole story. Functional potency data tells a different tale. The two molecules have similar EC50 values (around 11 nM for 11-OH-THC, 5.2 nM for Δ9-THC), and 11-hydroxy-THC actually produces a lower maximum response at the receptor than Δ9-THC does. So the popular claim that 11-OH-THC is “2 to 3 times more potent than THC” is a simplification. What’s really happening is that edibles produce a different profile of cannabinoids hitting your receptors, not just a stronger dose of the same thing.
Peak blood concentration of the combined Δ9-THC plus 11-OH-THC tends to hit 1 to 3 hours after you swallow. That’s the moment your friends notice you’ve stopped participating in the conversation. From there, the levels fall gradually over the next several hours. Effects usually last 4 to 8 hours, and can stretch to 10 to 12 hours at higher doses or with slower metabolism.
Why Oral Bioavailability Is So Low
Bioavailability is just a fancy word for “how much of what you consumed actually makes it into your bloodstream.” For smoked or vaporized THC, bioavailability averages around 30 percent. For oral THC in a capsule or edible, the number is much lower.
According to McGilveray’s 2005 review in Pain Research and Management, oral THC bioavailability ranges from about 4 to 12 percent, with high person-to-person variability. So if you swallow a 10mg gummy, somewhere between 0.4mg and 1.2mg of the parent Δ9-THC molecule actually reaches your blood. The rest is either never absorbed at all or gets destroyed by first-pass liver metabolism.
If that sounds terrible, keep in mind: first-pass also creates 11-hydroxy-THC, which wasn’t in your original gummy but now makes up a big share of the cannabinoid content in your bloodstream. That’s why oral THC still gets you high despite the miserable bioavailability number. You are feeling the combined effect of the surviving Δ9-THC plus the newly manufactured metabolite.
The practical implication is this: a 10mg edible and a 10mg vape puff are not the same dose. They deliver different amounts of the parent molecule and very different ratios of Δ9-THC to 11-OH-THC. This is why people who are comfortable with one format can get blindsided by the other.
How Food Changes Everything
If there’s one factor that can radically shift your edible experience, it is what else is in your stomach. And the research on this is pretty clear.
A 2019 study by Lunn and colleagues, published in Cannabis and Cannabinoid Research, gave 28 healthy adults (13 female, 15 male) 5mg or 10mg oral THC capsules under fasted and fed conditions. The fed condition was a standard high-fat breakfast. The results are the clearest answer we have to the “should I eat first?” question.
At a 5mg dose, the time to peak plasma concentration (Tmax) was:
- Fasted: about 1.9 hours
- Fed: about 6.6 hours
That’s a roughly 3.5-fold delay. Food also boosted total THC exposure (measured as area under the curve, or AUC) by about 2.7-fold at 5mg and 2-fold at 10mg. In other words, a meal makes the onset later but the total dose absorbed bigger. The peak blood concentration (Cmax) itself did not change significantly between fed and fasted.
Lunn’s team also found a sex difference at the 5mg fasted dose: females showed higher Cmax (2.36 ± 1.08 ng/mL) than males (1.39 ± 0.69 ng/mL). That difference was not observed at higher doses or in the fed condition.
The takeaway is useful. If you want faster onset and a shorter, lighter experience, eat an edible on an empty stomach and expect the hit in 60 to 90 minutes. If you want a slower onset with a bigger total exposure, eat it alongside or after a fatty meal and expect the hit at 2 to 4 hours with a longer tail. Pick one. Do not pick “eat with a light snack and see what happens” if you want predictability.
CYP2C9 Variability: Same Dose, Different People
You have a friend who eats 50mg gummies and watches a movie. Another friend took 5mg once and swore off edibles forever. Part of that difference is tolerance. A bigger part is often the gene that codes for CYP2C9.
CYP2C9 is the main enzyme responsible for converting Δ9-THC into 11-hydroxy-THC. Two common genetic variants of this enzyme, called CYP2C9*2 and CYP2C9*3, produce a less active version of the enzyme. If you inherit those variants, you metabolize THC more slowly. The parent Δ9-THC hangs around longer, clearance takes longer, and the whole experience gets stretched out and often feels more intense.
This isn’t small. Researchers who have studied oral THC pharmacokinetics in people with different CYP2C9 genotypes have found meaningful differences in peak concentrations and duration between “normal” metabolizers and slow metabolizers. There is no easy at-home test for this. You’d have to order pharmacogenomic panel testing to know your status.
The practical move: if edibles consistently feel much stronger than the milligrams on the label suggest, slow CYP2C9 activity is one of the possible explanations. Your dose is not the label dose. It’s the label dose filtered through your specific enzyme chemistry. Start with the lowest available strength and titrate up by 2.5mg increments over separate sessions until you find your baseline.
What THC Does to Your Gut Beyond Getting You High
Your digestive tract is not just a passive tube that THC travels through. It has its own population of cannabinoid receptors, which means THC is actively interacting with your gut before it even reaches your liver.
CB1 receptors are found throughout the enteric nervous system (the network of neurons lining your GI tract, sometimes called your “second brain”). When CB1 receptors activate, they slow down the release of neurotransmitters that drive gut motility. In plain terms: THC can slow your digestion down. That is why many people feel a subtle calm in their stomach after consuming cannabis, and it’s part of the mechanism behind prescription cannabinoid medicines used to reduce nausea.
CB1 receptors are also densely expressed in the lower esophagus. A 2023 Cureus literature review by Adenusi and colleagues compiled findings that chronic cannabis users tend to report more heartburn than non-users, and that CB1 activation at the lower esophageal sphincter can increase transient relaxations of that sphincter, letting stomach acid splash upward. For occasional users this is rarely noticed. For heavy daily users, it’s something to be aware of.
CB2 receptors are the other half of the story. In a healthy gut, CB2 receptors are quietly present on immune cells and some enteric neurons and don’t do much. When inflammation shows up, CB2 activity ramps up and tends to dampen the inflammatory response. This is why CB2-targeted cannabinoids are being studied for inflammatory bowel conditions.
One worth mentioning: chronic, heavy cannabis use in a small subset of users can trigger cannabinoid hyperemesis syndrome (CHS), a condition marked by cycles of severe nausea and vomiting that paradoxically gets temporary relief from hot showers. CHS is uncommon but real. If you experience cyclic vomiting that tracks with your cannabis use, it’s worth talking to a doctor.
The Enterohepatic Recirculation Loop
Here’s the plot twist that explains why edibles can feel like they come in waves. After your liver processes THC, some of the metabolites get excreted into your bile and dumped back into your small intestine. Once there, some of those metabolites are reabsorbed through the intestinal wall, travel back to the liver through the portal vein, and get processed again. This round trip is called enterohepatic recirculation.
The effect is a kind of drug recycling. Instead of getting one clean dose that peaks and clears, you get a prolonged exposure curve with subtle second-wave behavior. This is one of the reasons the total half-life of oral THC and its metabolites is measured in days for occasional users and weeks for heavy users.
For most people the enterohepatic loop is barely noticeable. If you’re paying attention, though, you may notice the high seems to resettle into you at the 4 to 5 hour mark, long after you thought it was fading. That’s likely a real pharmacokinetic event, not your imagination.
How Long THC Stays in Your Body After Digestion
Once digestion is done, the THC that did make it into your blood has to go somewhere. Because THC is fat-soluble, a lot of it ends up stored in adipose (fat) tissue, from which it slowly releases back into circulation over days and weeks. This is why cannabis has such a long detection window compared to most other drugs.
For a standard urine drug test, which looks for THC-COOH (the inactive metabolite your liver produces after 11-OH-THC), typical detection windows look roughly like this:
| Use Pattern | Typical Urine Detection Window |
| Single use / infrequent | 3 to 7 days |
| Moderate (a few times per week) | 7 to 21 days |
| Daily / heavy | 30 to 77 days |
The bulk of THC-COOH is excreted through feces (roughly two-thirds), with the rest leaving through urine. It doesn’t matter whether the original THC got into you via a gummy or a vape cartridge. Once it’s processed, it’s the same metabolite doing the same leaving.
If drug testing is on your radar, we cover the specifics in our guides on THCa and drug testing and whether CBD shows up on a drug test.
How to Time Edibles for the Best Experience
Everything above is academic until you actually have to decide what to eat, when to eat it, and how much. Here’s a practical playbook based on the digestive stages we just walked through.
If you want a faster, lighter experience
- Consume on a mostly empty stomach (2+ hours since your last meal)
- Expect onset in 45 to 90 minutes
- Start with 2.5 to 5mg if you’re new or sensitive
- Duration will generally be shorter, around 3 to 5 hours
If you want a slower, bigger, longer experience
- Eat an edible alongside a fatty meal (avocado, cheese, nut butter, full-fat yogurt)
- Expect onset in 2 to 4 hours (remember the Lunn 2019 Tmax delay)
- Be prepared for a higher total exposure even if the initial hit feels mild
- Duration can run 6 to 10+ hours
No matter what you do
- Wait a full 2 hours before taking more. This single rule prevents more bad trips than any other piece of advice
- Have CBD on hand. 25 to 50mg of CBD can help take the edge off if an edible hits harder than expected
- Know your product. Check the certificate of analysis for exact THC content. Homemade and unregulated edibles are notorious for inconsistent dosing
- Prefer a fast-acting format if you want predictability. THCa vapes and THCa flower skip the digestive system entirely and give you onset in 2 to 10 minutes with a clear 1 to 3 hour arc
Rule of thumb: You can always take more. You cannot take less. If you’re not sure, under-dose and wait.
Frequently Asked Questions
Because the THC has to travel through your stomach, your small intestine, and your liver before any of it reaches your brain. Gastric emptying alone can take 20 to 60 minutes on an empty stomach or 2 to 4 hours on a full one. Then absorption through the small intestinal wall and first-pass liver metabolism add more time. The typical onset window is 30 to 120 minutes, and food can push that to 4 hours or longer.
Barely. Your stomach is too acidic and has too small a surface area to absorb much fat-soluble compound. Its job is mechanical: break the edible down and hand the contents off to the small intestine. The small intestine is where almost all THC absorption actually happens, via chylomicrons and the portal venous blood.
11-hydroxy-THC is a metabolite your liver makes from Δ9-THC during first-pass metabolism, primarily via the CYP2C9 and CYP3A4 enzymes. It binds the CB1 receptor with much higher affinity than Δ9-THC (Ki around 0.37 nM vs 35 nM) and crosses the blood-brain barrier efficiently. Edibles produce much more 11-OH-THC than inhaled cannabis does, which is a big part of why edibles feel different from smoking.
Both, depending on how you measure. A 2019 study by Lunn and colleagues in Cannabis and Cannabinoid Research found that a high-fat meal delayed time to peak blood THC by about 3.5-fold at a 5mg dose (from 1.9 hours fasted to 6.6 hours fed) while increasing total exposure (AUC) by about 2.7-fold. So eating makes the onset later but the total dose absorbed bigger.
Several reasons, but the biggest single factor is variability in the CYP2C9 liver enzyme that metabolizes THC. Common genetic variants (CYP2C9*2 and *3) produce slower enzyme activity, which leads to higher blood concentrations and longer effects from the same dose. Body composition, recent meals, tolerance, and hydration also play roles, but genetics are often the hidden driver.
Occasionally, yes. CB1 receptors in the enteric nervous system can slow gut motility, and CB1 activation at the lower esophageal sphincter is associated with more heartburn in chronic users. In rare cases, heavy long-term cannabis use can trigger cannabinoid hyperemesis syndrome (CHS), a cyclic vomiting condition that resolves when cannabis is stopped. Most moderate users do not experience these issues.
Find Your Format at TribeTokes
Understanding what your gut, liver, and bloodstream are doing with THC is the difference between guessing and choosing. If you want the slower, body-heavy, longer arc of an edible, now you know why it takes its time. If you want predictable onset and easy titration, a vape or flower session skips the digestive system entirely and gives you a clear 2-to-10-minute window.
At TribeTokes, every product ships with third-party certificates of analysis so you know the exact THC content going in. Our THCa vape collection is built for precise dosing and fast onset. Our THCa flower comes from indoor-grown, hand-trimmed plants with full cannabinoid and terpene reporting.
If you want to go deeper on how all this fits together, read our full THC effects timeline or our primer on THCa vs THC.
Start low. Go slow. Enjoy the ride.
Shop TribeTokes THCa Vapes & Flower
Lab-tested, woman-owned since 2017. Precise dosing when you want predictable onset, premium indoor flower when you want the classic experience.